
Hyperbaric Oxygen Therapy Pros and Cons for Crush Injury: An Honest Patient Guide
Every patient evaluating HBOT for a crush injury deserves the same thing: the real pros, the real cons, and the honest context that lets them make an informed decision. Here is that conversation.
hyperbaric oxygen therapy pros and cons — crush injury patient guide reperfusion tissue salvage
The hyperbaric oxygen therapy pros and cons for crush injury are not evenly distributed — and that asymmetry is worth understanding clearly.
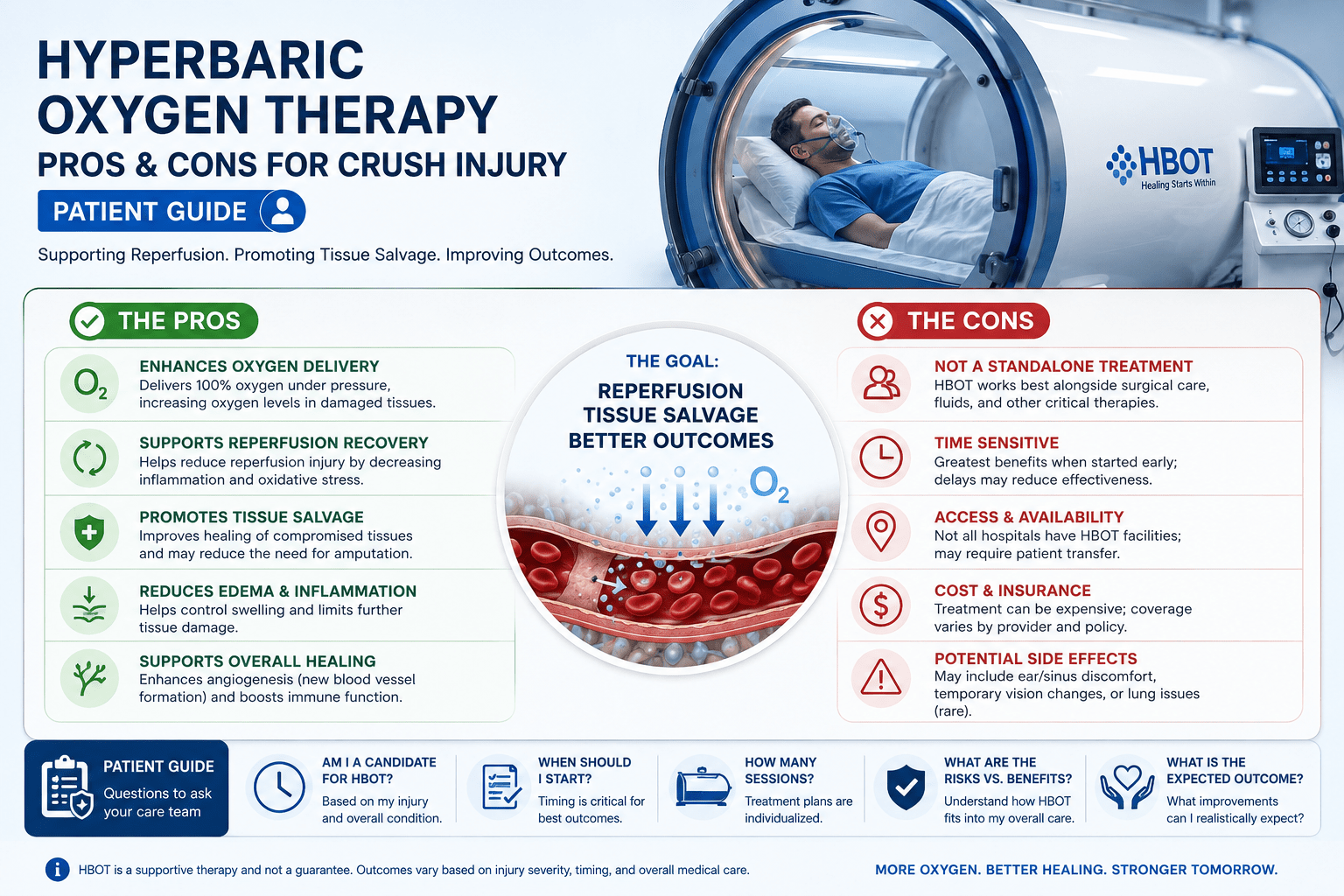
The pros are biological and documented: HBOT modulates reperfusion injury, preserves tissue that would otherwise die, accelerates wound healing, and reduces the need for repeat surgical debridement. These are mechanism-specific benefits with consistent evidence across clinical series.
The cons are practical rather than biological: timing constraints that make access in the six-hour window difficult, session requirements that demand sustained commitment, and limited facility availability that creates geography-dependent outcomes in India.
Understanding both sides of this equation is what allows patients, families, and the surgeons managing their care to make well-informed decisions — rather than being surprised by limitations they were not told about.
For the detailed evidence review, see our article on hyperbaric oxygen therapy reviews for crush injury. For the primary protocol guide, see HBOT for crush injury and compartment syndrome.
How to read this guide: The pros and cons below are separated into two categories — biological (what the therapy does and does not do at the cellular level) and practical (what makes it difficult to access and complete). Both matter. The biological pros are real but only realisable if the practical cons are addressed. A therapy that works but cannot be accessed in time delivers no benefit.
Hyperbaric Oxygen Therapy Pros for Crush Injury — The Documented Benefits
Pro 1 — Reperfusion Injury Modulation
The strongest and most consistently documented pro of HBOT for crush injury is its effect on reperfusion injury — the cascade of inflammatory damage that occurs when blood flow is restored to ischaemic tissue.
documented that HBOT inhibits neutrophil-endothelium adhesion — the cellular event that initiates the reperfusion injury inflammatory cascade. By intercepting this event within the first hours of reperfusion, HBOT reduces the zone of secondary tissue necrosis that standard surgical management cannot prevent.
This is the pro that matters most clinically: not just that HBOT helps wounds heal faster, but that it preserves tissue that would otherwise die regardless of surgical skill.
Pro 2 — Tissue Salvage in Limb-Threatening Injuries
Multiple clinical series document tissue salvage rates of 80 to 90% in limb-threatening crush injuries where HBOT was initiated within 6 hours, compared to 50 to 60% in comparable injuries without HBOT. For a patient facing potential amputation, this difference is the entire outcome.
The salvage benefit is most pronounced in injuries with a significant ischaemia-reperfusion component — which describes most high-energy crush injuries from road traffic accidents, industrial machinery, and building collapses.
Pro 3 — Plasma Oxygenation Without Functional Circulation
In the hours before and after vascular repair, HBOT delivers oxygen to ischaemic tissue through plasma dissolution — independent of the damaged microcirculation. This bridge oxygenation maintains tissue viability during the period when surgical restoration of flow is most critical.
Standard wound care cannot replicate this. No dressing, no topical agent, and no systemic medication reaches hypoxic tissue through plasma diffusion in the way HBOT does at therapeutic pressure.
Pro 4 — Oedema Reduction
HBOT produces vasoconstriction that reduces tissue oedema without compromising oxygenation — because the plasma oxygen concentration at 2.0 to 2.4 ATA compensates for the reduced blood flow. This oedema reduction is particularly valuable in compartment syndrome, where elevated compartment pressure is the direct mechanism of tissue ischaemia.
Pro 5 — Faster Wound Healing and Reduced Surgical Re-intervention
Beyond the acute phase, HBOT accelerates wound healing through angiogenesis — triggering new blood vessel growth in the traumatised tissue bed. Clinical series document reduced rates of repeat surgical debridement and earlier wound closure in crush injury patients who receive HBOT compared to those who do not.
| Pro | Biological Mechanism | Clinical Evidence Level | Magnitude of Benefit |
| Reperfusion injury modulation | Neutrophil adhesion inhibition; ROS cascade reduction | Strong — mechanistic + clinical series | Reduces secondary necrosis zone by documented margin |
| Tissue salvage | Plasma O₂ + reperfusion modulation combined | Strong — comparative clinical series | 80–90% vs 50–60% salvage in limb-threatening injuries |
| Bridge oxygenation | Plasma O₂ diffusion independent of circulation | Strong — mechanism documented; clinical benefit consistent | Maintains viability through surgical repair window |
| Oedema reduction | Vasoconstriction with maintained plasma O₂ | Moderate — clinical observation; mechanism confirmed | Reduces compartment pressure; improves surgical conditions |
| Wound healing acceleration | Angiogenesis; fibroblast activation | Strong — multiple wound healing series | Faster closure; reduced debridement requirement |
Hyperbaric Oxygen Therapy Cons for Crush Injury — The Honest Limitations
Con 1 — The Six-Hour Window Is Often Missed
The single most important limitation of HBOT for crush injury is the same as its most important advantage: timing. The reperfusion injury modulation benefit is maximised within 6 hours of injury. Most Indian tertiary trauma centres do not have on-site hyperbaric facilities. Transfer time between a trauma centre and a hyperbaric facility — added to the time for initial surgical stabilisation — frequently exceeds 6 hours.
This is not a biological limitation of HBOT. It is a structural limitation of Indian healthcare delivery. The therapy works in the window. The window closes before the therapy can be initiated in most cases.
Con 2 — Session Commitment
A standard HBOT course for crush injury requires 10 to 20 sessions — one to two sessions per day in the acute phase, then once daily as the course continues. Each session is 90 minutes inside the chamber. For patients managing a serious trauma injury, the physical and logistical demands of this schedule are substantial.
Incomplete courses — stopped at session 8 or 10 because the patient or family found the commitment unsustainable — produce partial results. The angiogenesis benefit that drives long-term tissue recovery accumulates over the full course. Stopping early means stopping before the benefit has fully established.
Con 3 — Limited Facility Access in India
Hyperbaric facilities capable of treating acute crush injury at the required pressure (2.0 to 2.4 ATA) and with adequate staffing for critically ill patients are available in Delhi NCR, Mumbai, Bangalore, Hyderabad, and Chennai — and in limited number outside these metros. For patients injured in smaller cities, on highways, or in agricultural areas, the nearest qualified facility may be several hours away.
This is the practical con that most significantly limits HBOT outcomes for crush injury in India. The therapy is available. It just is not available where the injuries happen.
Con 4 — Side Effects That Require Management
HBOT’s side effects are manageable but real. Ear and sinus barotrauma affect approximately 2% of sessions — painful for patients who cannot equalise, particularly those with facial or head injuries. Oxygen toxicity seizures affect fewer than 1 in 10,000 sessions but require monitoring protocols. For crush injury patients already dealing with significant pain, the additional demands of chamber-related discomfort are a genuine consideration. The full side effect profile is covered in our article on hyperbaric oxygen therapy side effects.
Con 5 — Not Effective for All Injury Types
HBOT is most effective for crush injuries with a significant ischaemia-reperfusion component. High-velocity penetrating injuries, crush injuries with immediate surgical revascularisation and minimal ischaemia time, and injuries where the primary damage is structural rather than vascular may have less pronounced HBOT benefit. The indication is specific — and the benefit is proportionate to the degree of reperfusion injury in the individual case.
The honest pros and cons of HBOT for crush injury are not difficult to summarise. The biology is strongly in favour. The practical infrastructure in India is the limitation. Improving outcomes means closing the gap between where the therapy works and where the injuries happen.
hyperbaric oxygen therapy pros and cons — six hour window tissue salvage crush injury access India
Pros and Cons Balanced: Who Should Pursue HBOT for Crush Injury
Given the documented pros and the practical cons, the patients most likely to achieve the full tissue salvage benefit are those where the practical cons can be minimised.
| Ideal Candidate Profile | High-energy crush injury with significant soft tissue involvement and ischaemia-reperfusion component. Located within 3 hours of a qualified hyperbaric facility at the time of injury. Medically stable enough for chamber entry within 6 hours of surgical stabilisation. Able to commit to daily sessions for 2 to 3 weeks post-injury. No absolute contraindications (pneumothorax, specific chemotherapy agents). |
For patients who do not fit this profile — injury too remote from a facility, or presentation too delayed — HBOT still offers benefit in the wound healing and infection management phases, even if the acute reperfusion injury window has passed. The full tissue salvage benefit requires early initiation. The wound healing benefit is available throughout the recovery course.
Addressing the Cons — What the India Context Requires
The practical cons of HBOT for crush injury in India are not arguments against the therapy. They are arguments for infrastructure investment — and for changing the way referral decisions are made.
- Earlier referral decisions: HBOT referral should be made in parallel with surgical planning, not after recovery. The six-hour window requires a parallel decision-making process, not a sequential one.
- Advance facility identification: trauma centres should have established referral pathways to the nearest hyperbaric facility — contact numbers, transport protocols, and pre-authorisation for emergency transfers.
- Patient education on session commitment: before starting, patients and families should understand the full course requirement and plan for it logistically. Dropping out at session 10 is the most common cause of suboptimal outcomes.
For HBOT facility locations in India, see our guides to HBOT in Delhi and HBOT in Bangalore. For a complete national access guide, see our HBOT near me India guide. For insurance guidance, see our HBOT insurance India guide.
Frequently Asked Questions
Is the risk of HBOT worth it for crush injury?
For limb-threatening crush injuries with a significant reperfusion component — yes, the benefit-risk ratio strongly favours HBOT. The risk of serious adverse events is less than 1 in 10,000 sessions. The tissue salvage benefit in appropriate candidates is documented at 80 to 90% compared to 50 to 60% without HBOT. For a patient facing potential amputation, that difference is not marginal.
What if I cannot access HBOT within 6 hours?
Initiate HBOT as soon as it is accessible — even beyond the 6-hour window. The reperfusion injury prevention benefit diminishes significantly after 12 hours, but the wound healing, oedema reduction, and infection management benefits remain available throughout the recovery course. A course started at 24 hours post-injury still reduces repeat debridement rates and accelerates wound closure — the outcome is different from early initiation but meaningfully better than no HBOT.
Can HBOT cause additional damage to crush-injured tissue?
No — at therapeutic pressures (2.0 to 2.4 ATA), HBOT does not cause additional tissue damage. The theoretical concern about oxygen toxicity is managed through standard protocol air breaks. The vasoconstriction produced by HBOT is offset by the increased plasma oxygen concentration — tissue oxygen delivery is maintained or improved despite reduced blood flow. Concerns about HBOT worsening crush injury outcomes are not supported by the evidence.
How does HBOT compare to other adjunctive treatments for crush injury?
HBOT is the only adjunctive therapy with documented evidence for reperfusion injury modulation at the cellular level for crush injury. Negative pressure wound therapy supports wound healing but does not address the reperfusion cascade. Systemic anti-inflammatory medications reduce inflammation broadly but cannot deliver therapeutic oxygen to hypoxic tissue. HBOT’s mechanism is specific to the biological problem that crush injury creates — it is not interchangeable with other adjuncts.
Is HBOT covered by insurance for crush injury in India?
Coverage varies by policy and indication. For current guidance on insurance coverage for HBOT in India across indications, see our HBOT insurance India guide.
The Pros Win — If the Practical Cons Can Be Addressed
The pros and cons of hyperbaric oxygen therapy for crush injury resolve to a clear conclusion: the biology strongly favours HBOT for the right indication in the right time window. The practical cons — timing, access, commitment — are real, but they are surmountable with planning.
For patients managing a crush injury in India right now: understand the six-hour window, know where your nearest chamber is, and build the session commitment into your recovery plan from the beginning. The therapy works. The limiting factor is whether it can be reached in time and completed in full.
For surgeons and trauma physicians: the referral decision belongs in the same conversation as the surgical plan — not after it. The pros of HBOT for crush injury are maximised when the practical cons are anticipated and addressed from the first hour.
The tissue salvage data for HBOT in crush injury is among the most compelling in emergency medicine. 80–90% vs 50–60% — that gap is the documented consequence of whether reperfusion injury modulation is initiated in time. The therapy is available. The window is manageable with planning. The pros of starting in time substantially outweigh every practical con of accessing and completing the course.
For the full crush injury protocol and evidence, see our primary guide on HBOT for crush injury and compartment syndrome. For the complete 14-indication overview, see our HBOT uses guide.
The pros are documented. The cons are practical. The decision is about planning, not biology.




