
Gas Gangrene Survivors: What HBOT Did When Surgery Alone Was Not Enough
The preferred treatment for gas gangrene is not surgery. It is not antibiotics. It is the combination of surgery, antibiotics, and HBOT — all three, simultaneously. This is the UHMS standard of care, not an experimental suggestion.
 HBOT gas gangrene treatment — hyperbaric oxygen therapy clostridial myonecrosis
HBOT gas gangrene treatment — hyperbaric oxygen therapy clostridial myonecrosis
Gas gangrene does not wait.
There is no condition in medicine that moves faster through tissue. Clostridial myonecrosis — the clinical name for gas gangrene — can destroy muscle at a rate visible to the naked eye. What looks like a contained wound at midnight can be a life-threatening emergency by morning.
If you are reading this because someone you love is facing this diagnosis — a family member post-surgery, post-trauma, post-crush injury — you are already in the hardest possible position. The decisions are being made fast. The clinical language is unfamiliar. And you need to understand one thing above all else.
Surgery alone is not enough. Antibiotics alone are not enough. What the evidence and the clinical standard of care are clear about is this: the combination of surgery, antibiotics, and HBOT gives the best chance of survival and the best chance of preserving the limb — and the three must work together, not sequentially.
Here is why HBOT is not the last resort. It is the third pillar of a complete treatment. And understanding this changes how you advocate for the person in that hospital bed.
What Gas Gangrene Is — Speed, Mechanism, and Why It Is Different From Other Infections
Clostridial Myonecrosis — The Biological Explanation
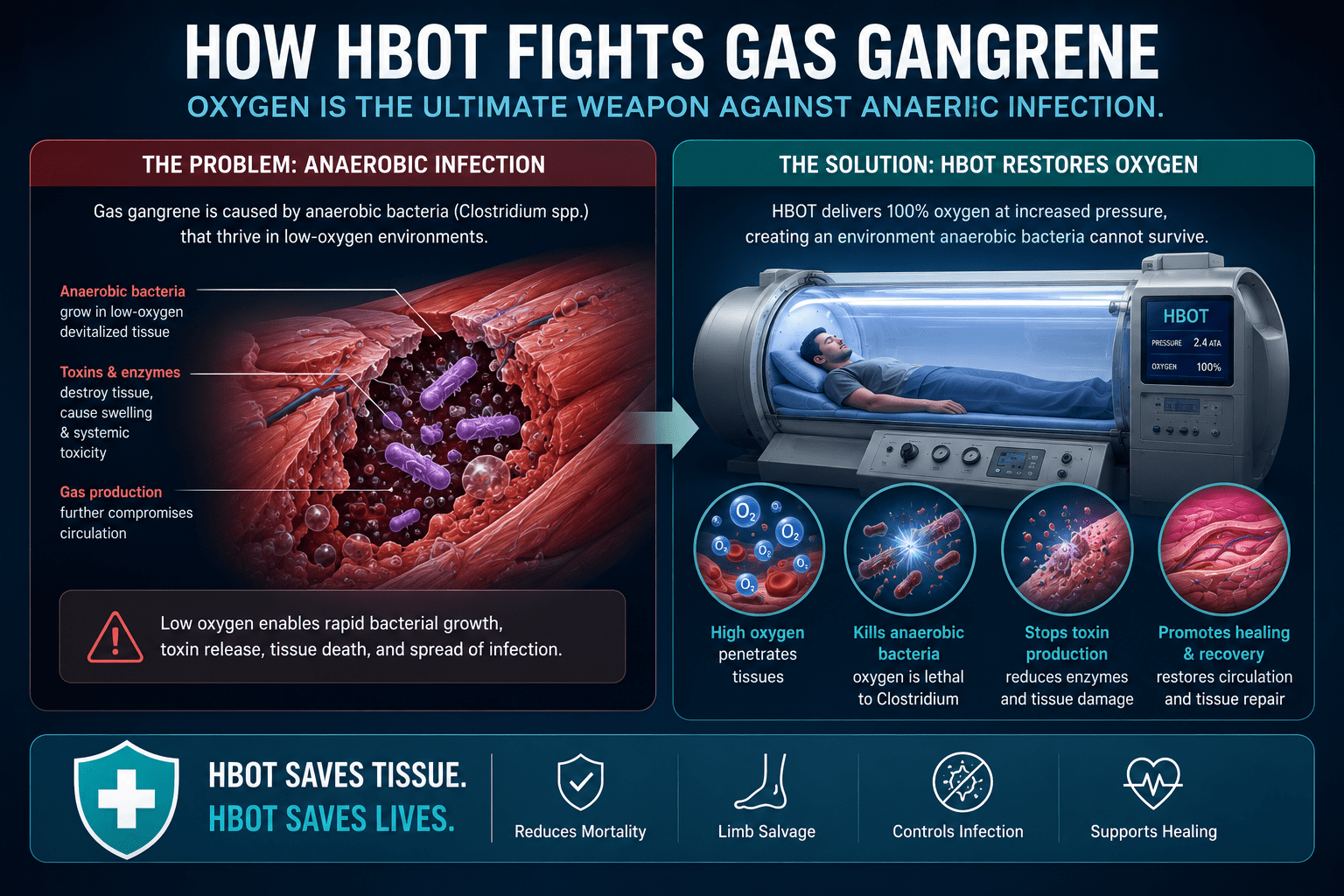
Gas gangrene is caused by Clostridium bacteria — most commonly Clostridium perfringens — anaerobic organisms that thrive in oxygen-deprived environments. They are present in soil, in the human gut, and on the surface of skin. Under normal circumstances, they are harmless. When they reach deep tissue — through trauma, surgery, injection, or devascularisation — they find exactly the environment they need.
The tissue they colonise is already hypoxic. The wound is already compromised. And what these bacteria do in that environment is uniquely destructive: they produce alpha-toxin, a lecithinase that destroys cell membranes. They produce gas — hydrogen, carbon dioxide — that spreads through fascial planes, driving the infection further and faster than any other bacteria in clinical medicine.
The gas you can feel crackling under the skin in a gas gangrene patient is not incidental. It is a diagnostic sign of active bacterial toxin production happening right now, in the tissue beneath your hand.
Why It Spreads Faster Than Surgery Can Follow
A standard surgical debridement removes what is visibly necrotic. But gas gangrene spreads through fascial planes — the connective tissue that surrounds and separates muscle groups — faster than tissue death creates visible demarcation. The surgeon debrides the dead tissue. The bacteria are already 5 centimetres further along in tissue that looks healthy under the blade.
This is the fundamental limitation of surgery alone. It is reactive. It removes what has already died. It cannot stop what is currently dying.
That is what HBOT addresses.
| Treatment | What It Targets | What It Cannot Address |
|---|---|---|
| Surgery | Dead and grossly infected tissue — removal prevents local spread | Bacteria already in viable tissue beyond the surgical margin; toxin already circulating |
| Antibiotics | Bacterial protein synthesis and cell wall — systemic antimicrobial action | Hypoxic tissue where antibiotic penetration and efficacy are impaired; anaerobic bacterial populations |
| HBOT | Anaerobic bacteria directly — oxygen is lethal to their metabolism; toxin production halted | Tissue that is already necrotic — HBOT works at the margin, not on dead tissue |
Why HBOT Works Against Gas Gangrene — The Anaerobic Vulnerability
This is the mechanism that makes HBOT not just useful but biologically irreplaceable in gas gangrene treatment.
Clostridium bacteria are obligate anaerobes. They cannot survive in oxygen-rich environments. Their entire metabolism — energy production, toxin synthesis, cell replication — depends on the absence of oxygen. This is not a weaknesses among others. It is the fundamental constraint of their biology.
HBOT removes that constraint from the infected tissue.
What Happens at 2.0–2.5 ATA
At 2.0 to 2.5 atmospheres absolute, tissue oxygen tension rises to levels to be directly lethal to Clostridial species. This is not a recent finding — it is the foundational research that established HBOT as a clinical treatment for gas gangrene more than five decades ago. The biology has not changed.
Alpha-toxin production halts within the first HBOT session. Bacterial replication in oxygenated tissue stops. The spread through fascial planes — the characteristic that makes gas gangrene so devastating — is arrested because the environment those bacteria require no longer exists in the treated tissue.
Tissue Margin Preservation — The Clinical Consequence
When bacterial spread halts and toxin production stops, something clinically critical becomes possible: the tissue at the margin of the infection — the tissue that is hypoxic and at risk but not yet necrotic — can be preserved.
This margin preservation is what changes amputation outcomes. confirmed that HBOT as an adjunct to surgery and antibiotics for clostridial infection reduces the extent of surgical debridement required — because the infection is arrested before more tissue crosses the threshold from viable to dead.
Surgery removes less. The patient keeps more. This is the direct clinical benefit of adding HBOT to the protocol.
Immune Enhancement in Hypoxic Tissue
Gas gangrene tissue is profoundly hypoxic. The immune response — leukocyte killing of bacteria — requires oxygen to function. Neutrophils in oxygen-deprived tissue cannot mount the oxidative burst that kills bacteria effectively, regardless of how many of them arrive at the infection site.
HBOT restores the oxygen gradient that immune function requires. confirmed that leukocyte bacterial killing capacity is significantly enhanced by HBOT-induced tissue oxygenation — turning a dysfunctional immune environment into one capable of supporting the antimicrobial activity that the infection demands.
 HBOT gas gangrene — anaerobic bacteria oxygen lethality mechanism
HBOT gas gangrene — anaerobic bacteria oxygen lethality mechanism
What the Clinical Evidence Shows — Survival and Limb Preservation
Gas gangrene is rare enough that randomised controlled trials are not ethically feasible — you cannot withhold a potentially life-saving treatment to create a control group. The evidence base is built from retrospective series, cohort studies, and decades of clinical experience.
What that evidence consistently shows is this:
| Mortality Evidence | A retrospective study examining ineligibility for HBOT despite clinical indication in necrotising soft tissue infections — the category that includes gas gangrene — found an odds ratio of 8.59 for mortality in patients who could not receive HBOT. The inverse signal is consistent: patients who receive HBOT as part of the complete protocol have significantly better survival outcomes than those who do not. |
| UHMS Standard | The Undersea and Hyperbaric Medical Society (UHMS) classifies clostridial myonecrosis as a primary indication for HBOT — not an optional add-on but a core component of the standard treatment protocol. The evidence threshold for inclusion in the UHMS indications list is among the highest in hyperbaric medicine. |
What HBOT Changes in Practice
- Number of surgical debridements required: Reduced — because HBOT arrests bacterial spread at the margin, less tissue crosses from viable to necrotic between surgical sessions
- Amputation rate: Lower in HBOT-treated patients — margin preservation translates directly to limb salvage in cases where the infection borders critical anatomical structures
- Time to infection control: Accelerated — the combination of direct bacterial killing, toxin suppression, and immune enhancement works faster than antibiotics and surgery alone
- Recovery trajectory: Improved — surviving patients who received HBOT show better functional outcomes because more viable tissue was preserved during the acute phase
What the HBOT Protocol Looks Like in Gas Gangrene Treatment
Session Parameters
- Pressure: 2.0 to 2.5 ATA — the range that achieves lethal tissue oxygen tension for Clostridial species
- Duration: 90-minute sessions
- Frequency: Three sessions in the first 24 hours — the highest session density used in any HBOT indication, reflecting the urgency of the infection
- Subsequent days: Two sessions per day until infection is controlled and the patient is stabilising
- Total course: Typically 7 to 10 sessions; severe cases may require more
Sequencing With Surgery and Antibiotics
The critical point about gas gangrene management is that HBOT is not started after surgery and antibiotics have had their chance. It is started concurrently — as part of the same acute management plan.
- Initial surgical debridement — removes grossly necrotic tissue and reduces bacterial load
- High-dose broad-spectrum antibiotics — particularly penicillin G for Clostridium perfringens, with metronidazole for anaerobic coverage
- HBOT first session — within hours of diagnosis, not days; the first session begins halting toxin production and oxygenating the tissue margin
- Second surgical assessment — often reveals that the infection margin has stopped advancing; further debridement is more limited
- Continued HBOT and antibiotic course — until clinical and laboratory markers confirm infection control
Starting HBOT after surgery has failed is not the correct sequence. Starting HBOT alongside surgery — so that the infection is being addressed at the tissue level while the surgeon addresses the necrotic tissue — is what the evidence supports.
Who Benefits From HBOT in Gas Gangrene — Patient Profiles
Primary Indication — Confirmed or Suspected Gas Gangrene
- Any patient with confirmed or strongly suspected clostridial myonecrosis based on clinical signs — crepitation, rapid spread, characteristic wound odour, gas on imaging
- Post-traumatic wounds with contamination by soil, faeces, or foreign material in deep tissue
- Post-surgical wounds with rapid deterioration, particularly bowel surgery or lower limb vascular procedures
- Injection site infections with features of gas production in the tissue
Settings Where HBOT Access Must Be a Priority
- Tertiary hospitals managing major trauma — gas gangrene is a trauma complication; having HBOT available within the facility or a clear rapid-transfer protocol is a clinical quality standard
- Hospitals managing post-surgical complications — particularly after colorectal, orthopaedic, and vascular procedures
- Burn centres — deep burns with soil contamination carry Clostridial risk
Gas Gangrene in the Indian Clinical Context
India’s epidemiological profile for gas gangrene differs from Western settings in important ways. Agricultural injuries — penetrating wounds contaminated with soil — are a significant and underreported cause. Post-injection abscess complications, particularly in rural settings where injection technique and equipment sterility may be suboptimal, represent another distinct risk category.
The challenge in India is not the absence of surgical skill. Major trauma centres in Delhi, Mumbai, Bangalore, Hyderabad, and Chennai have the surgical capability to manage gas gangrene. The challenge is the absence of HBOT as a standard co-treatment option within or adjacent to these centres — and the absence of clinical protocols that trigger early HBOT referral at the time of diagnosis rather than after surgical options have been exhausted.
For HBOT availability in Indian cities, see our and our guide to .
Frequently Asked Questions
Is HBOT experimental for gas gangrene?
No. Gas gangrene — clostridial myonecrosis — has been a recognised indication for HBOT since the 1960s. The UHMS includes it in the primary indications list, which requires a substantial evidence base for inclusion. The mechanism is well understood, the clinical evidence is consistent, and international guidelines across North America, Europe, and Australia all include HBOT as a standard component of gas gangrene treatment.
What if the hospital treating the patient does not have HBOT?
This is the most common challenge in Indian clinical settings. The answer is not to proceed without HBOT — it is to initiate rapid transfer to a facility with HBOT capability, or to arrange temporary stabilisation while HBOT access is secured. Antibiotics and initial debridement can begin immediately. HBOT should follow within hours, not days. The hospital’s intensive care physician or surgical team should contact the nearest hyperbaric facility at the time of diagnosis.
Can HBOT prevent amputation in gas gangrene?
In many cases, yes — HBOT’s margin preservation effect directly reduces amputation rates. By halting bacterial spread at the infection margin, HBOT reduces the amount of viable tissue that crosses into necrosis between surgical debridements. The clinical literature consistently shows lower amputation rates in patients who received the complete three-pillar protocol compared to those who received surgery and antibiotics alone. No guarantee is possible in individual cases — but the population-level signal is consistent and clinically meaningful.
How quickly must HBOT begin to be effective?
The earlier the better. Gas gangrene is an infection measured in hours, not days. The first HBOT session should begin within hours of diagnosis — not after a second debridement, not the following morning. The goal is to halt toxin production and begin oxygenating the tissue margin before the infection has had another 12 hours to advance. Treatment protocols specify three sessions within the first 24 hours, reflecting the time-critical nature of the intervention.
Is HBOT safe in a critically ill patient?
Yes — with appropriate monitoring. HBOT is used routinely in patients with sepsis, multi-organ involvement, and mechanical ventilation. Modern hyperbaric chambers are designed for critical care patients and can accommodate monitoring equipment and ventilators. The risk-benefit calculation in a confirmed gas gangrene case strongly favours HBOT: the risk of the infection without HBOT significantly outweighs the manageable risks of hyperbaric treatment in a critically ill patient.
Three Treatments. One Standard. Better Outcomes.
Gas gangrene is one of the clearest examples in all of medicine of a condition where the sum of three treatments is greater than the sum of their individual parts.
Surgery removes what is dead. Antibiotics suppress what is alive. HBOT removes the environment that keeps the bacteria alive — and in doing so, protects the tissue that has not yet been lost.
If someone you care for is facing this diagnosis, the most important thing you can do — beyond trusting the surgical team — is to ask this question:
“Is HBOT being coordinated as part of the treatment protocol — not after surgery, but alongside it?”
That question is not a challenge to the clinical team. It is informed advocacy. And it may change the outcome.
To understand the full mechanism of how HBOT works at the biological level, visit . For the complete conditions evidence base, explore our .
For HBOT cost and session information, see our guide on .
The third pillar of treatment is not optional. Ask for it.



3 Comments
Comments are closed.


[…] For the related evidence on HBOT in gas gangrene — which shares the same anaerobic mechanism — see our article on gas gangrene and HBOT. […]
[…] the full clinical evidence on gas gangrene and HBOT outcomes, see our primary guide on HBOT for gas gangrene and clostridial myonecrosis. For the foundational oxygen delivery mechanism, visit How HBOT […]
[…] For the gas gangrene mechanism and evidence, see our guide on HBOT for gas gangrene and clostridial myonecrosis. […]