

The Silent Killer and the Only Treatment That Protects Your Brain
Delayed neurological sequelae occur in CO poisoning even after apparent recovery. Patients who received HBOT within 200 minutes of CO exposure had an odds ratio of 18.97 lower risk of delayed brain damage compared to those treated later.
 carbon monoxide poisoning HBOT treatment — hyperbaric oxygen brain protection
carbon monoxide poisoning HBOT treatment — hyperbaric oxygen brain protection
You survived the carbon monoxide. The question — and the doctors know it — is whether your brain did.
That sentence is not meant to alarm you unnecessarily. It is meant to tell you something that most people who survive CO poisoning are never clearly told: the neurological danger does not end when the gas leaves your blood.
Carbon monoxide poisoning is widely understood as an oxygen displacement event. You breathe in CO, it binds to your haemoglobin, your blood cannot carry oxygen, you lose consciousness, you are treated and discharged. The story seems to end there.
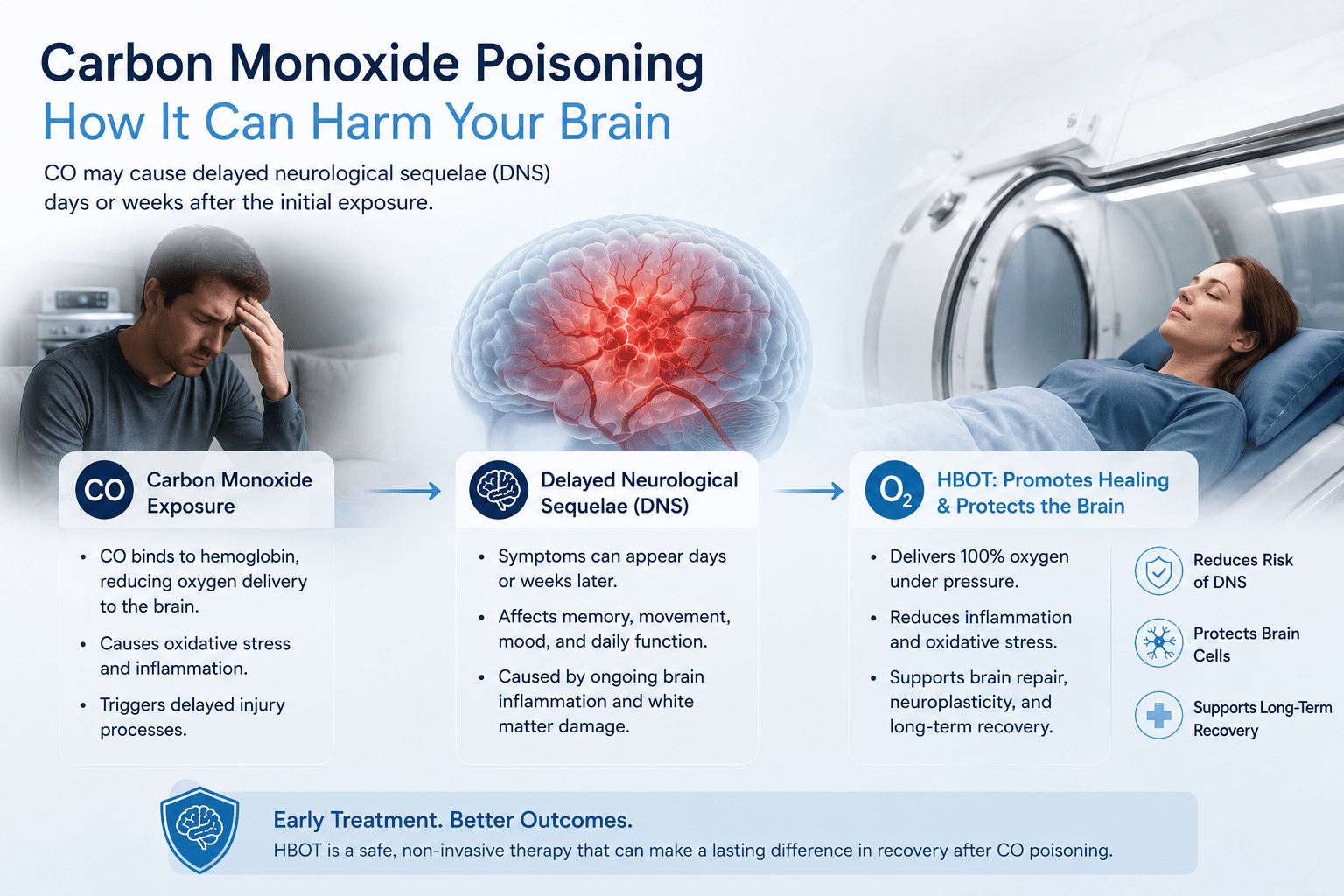
For many patients, it does not. Weeks after apparent recovery — sometimes while feeling completely well — memory lapses, confusion, personality changes, and cognitive decline begin to surface. This is delayed neurological sequelae (DNS). It is documented. It is predictable. And it is significantly more preventable than most patients and families ever know.
HBOT is the intervention that changes this. Not because it simply replaces the oxygen CO stole. But because it interrupts a neurological damage cascade that standard oxygen therapy cannot reach.
What Carbon Monoxide Does to the Body — Beyond the Textbook
The Haemoglobin Story Everyone Knows
Carbon monoxide binds to haemoglobin with approximately 200 times the affinity of oxygen. When you breathe CO, it displaces oxygen on haemoglobin molecules — forming carboxyhaemoglobin (COHb) — leaving the blood unable to carry oxygen to tissues. The brain and heart, being the most oxygen-dependent organs in the body, suffer first and most severely.
This is the mechanism most people learn. And it is real. But it is only part of what is happening.
The Neurological Story Most People Never Hear
The critical insight documented by is this: COHb levels do not correlate with the development of neurological or cognitive sequelae. A patient with a relatively low COHb level can develop severe DNS. A patient with a very high level may not. The toxic damage to the brain is not simply a function of how much CO bound to haemoglobin.
CO poisoning triggers a complex cascade of neurological damage that is independent of the haemoglobin-binding mechanism. The two organ systems most susceptible are the cardiovascular and central nervous systems — and the injury pathways involve multiple simultaneous processes.
| Damage Mechanism | What Happens | Standard O₂ Addresses This? |
|---|---|---|
| COHb formation | Oxygen displaced from haemoglobin; tissue hypoxia | Partially — accelerates CO elimination |
| Oxidative stress cascade | Reactive oxygen species damage neurons and vascular endothelium | No — requires pressure to interrupt |
| Neuroinflammation | Neutrophil and macrophage activation causes secondary brain injury | No — HBOT specifically reduces this |
| Mitochondrial dysfunction | CO binds to cytochrome c oxidase; cellular energy production fails | No — requires hyperoxic environment |
| Lipid peroxidation | Cell membrane destruction in neurons; delayed death of brain cells | No — HBOT interrupts peroxidation cascade |
| Perivascular injury | Blood vessel lining damage triggers delayed neurological deterioration | No — requires HBOT’s anti-inflammatory action |
COHb level does not predict neurological outcome. The brain damage from CO poisoning is driven by a cascade of mechanisms that begin during exposure and continue for weeks after CO clears from the blood.
Delayed Neurological Sequelae — The Second Wave of CO Damage
Delayed neurological sequelae (DNS) is the term for cognitive and neurological symptoms that emerge days to weeks after apparent recovery from CO poisoning — in patients who seemed to have fully recovered initially.
What DNS Looks Like
- Memory impairment — difficulty forming new memories or recalling recent events
- Cognitive decline — slower processing, reduced concentration, difficulty with complex tasks
- Personality changes — irritability, emotional dysregulation, apathy
- Parkinsonism — rigidity, tremor, bradykinesia emerging weeks after poisoning
- Urinary incontinence or gait disturbance in severe cases
- Depression and anxiety that appears to have no prior history
DNS is not rare. It occurs in a significant proportion of CO poisoning survivors, particularly those with loss of consciousness at the time of exposure or those with delayed access to treatment.
A 2024 prospective study published in enrolled 167 CO poisoning patients and analysed risk factors for DNS. The findings were striking: patients with a Glasgow Coma Scale score ≤9 at presentation had an odds ratio of 5.06 for developing DNS. But the more actionable finding concerned timing.
| Critical Research Finding | Patients who received HBOT 200 minutes or more after CO exposure had an odds ratio of 18.97 for developing delayed neurological sequelae — compared to those treated within 200 minutes. The AUC for this predictive model was 0.8235. Time to treatment is the most controllable risk factor for DNS. (Choi S et al., MDPI Diagnostics, January 2024) |
Why HBOT Protects the Brain — The Mechanisms Standard Oxygen Cannot Replicate
Standard oxygen therapy — a mask delivering 100% O₂ at normal atmospheric pressure — reduces CO half-life from approximately 5 hours to around 60 to 90 minutes. This is meaningfully helpful. It is not sufficient.
The neurological damage cascade described above is not driven by the presence of CO in the blood. It has already been triggered. It continues independently. And it requires mechanisms that atmospheric oxygen cannot provide.
Mechanism 1 — Accelerated CO Elimination at Pressure
At 2.4 ATA, HBOT reduces CO half-life to approximately 20 to 30 minutes — roughly three times faster than standard 100% oxygen therapy and more than ten times faster than breathing room air. Faster CO elimination means less cumulative exposure to COHb-mediated hypoxia during the critical early window.
Mechanism 2 — Interrupting the Oxidative Stress Cascade
As documented by , oxidative stress is fundamental to the mechanism of HBOT — and by extension, fundamental to CO poisoning treatment. HBOT at therapeutic pressure modulates reactive oxygen species signalling, reducing the cascade of lipid peroxidation and neuronal membrane damage that continues in the brain for days after CO exposure.
Mechanism 3 — Reducing Neuroinflammation
CO poisoning triggers neutrophil sequestration in the brain’s microvasculature — one of the primary drivers of secondary neurological injury. HBOT directly reduces neutrophil adhesion to damaged endothelium, interrupting the inflammatory process before it causes irreversible perivascular and neuronal damage.
established that this anti-inflammatory action — distinct from oxygen replacement — is one of HBOT’s most clinically significant contributions in CO poisoning management.
Mechanism 4 — Restoring Mitochondrial Function
CO binds to cytochrome c oxidase — the final enzyme in the mitochondrial electron transport chain — disrupting cellular energy production at the most fundamental level. This binding persists even after CO clears from haemoglobin.
HBOT at hyperoxic pressure displaces CO from cytochrome c oxidase and restores the electron transport chain’s function — directly addressing the cellular energy failure that standard oxygen therapy cannot correct. This mechanism was confirmed in mitochondrial protection research documented by
carbon monoxide poisoning HBOT brain protection — delayed neurological sequelae mechanism
Who Needs HBOT After CO Poisoning — Clinical Criteria
Not all CO poisoning survivors require HBOT. The following clinical criteria guide the decision:
Strong Indications for HBOT After CO Poisoning
- Loss of consciousness at any point during or after CO exposure
- Neurological symptoms — confusion, cognitive impairment, focal deficits — present at time of evaluation
- Cardiovascular involvement — ECG changes, ischaemic chest pain, elevated troponin
- COHb level ≥25% (lower thresholds apply in vulnerable populations)
- Pregnancy — HBOT is specifically recommended for pregnant patients with CO exposure due to foetal susceptibility
- Paediatric patients — children are disproportionately vulnerable to CO-mediated neurological damage
- Severe exposure with prolonged duration — even if COHb on arrival appears lower due to pre-hospital oxygen
Presentations Where HBOT Should Be Seriously Considered
- Any CO exposure with headache, nausea, or vomiting — even if COHb appears mild on arrival
- Patients with underlying cardiac or neurological conditions
- Patients in whom DNS risk is considered high based on exposure history
Important: COHb level measured at hospital arrival may significantly underestimate peak exposure if pre-hospital oxygen was administered during transport. Exposure history and clinical presentation should guide HBOT decision-making — not COHb alone.
Carbon Monoxide Poisoning in India — A Risk Hidden in Plain Sight
India’s CO poisoning risk profile is distinct from Western countries — and in many ways more acute. The sources are embedded in daily domestic life.
The Primary CO Sources in Indian Homes
- Diesel generators during power cuts — running indoors or in attached spaces is the most common cause of severe CO poisoning in Indian urban settings
- Gas geysers with inadequate ventilation — enclosed bathrooms with insufficient air exchange are a well-documented risk. Bathroom CO poisoning is frequently misidentified as cardiac or neurological events in Indian emergency rooms
- Coal and wood-burning cooking stoves — particularly in rural areas with unvented kitchen spaces
- Vehicle exhaust in enclosed garages — accidental and intentional, both significant in the Indian context
- Blocked or poorly maintained chimneys — seasonal risk in North India during winter months when heaters and fireplaces are used heavily
CO poisoning is significantly undercounted in Indian hospital data. The presenting symptoms — headache, nausea, dizziness, confusion — overlap completely with heat exhaustion, viral illness, and food poisoning. Without a CO detector in the home or a high index of clinical suspicion, the diagnosis is frequently missed.
This matters because every hour of diagnostic delay is an hour in which the neurological damage cascade is progressing without HBOT intervention.
| CO Detection in India | Carbon monoxide detectors are inexpensive (Rs. 1,500–3,500), widely available online, and capable of preventing the majority of accidental CO poisoning deaths. They are standard in most developed countries. In India, their adoption remains extremely low. A CO detector near the generator, water heater, and sleeping areas is among the highest-value safety investments an Indian household can make. |
What HBOT for CO Poisoning Looks Like — Protocol and Timeline
Standard HBOT Protocol for CO Poisoning
- Pressure: 2.4 to 3.0 ATA depending on severity
- Duration: 90-minute oxygen breathing sessions
- Frequency: One to three sessions in the first 24 hours for severe cases
- Repeat sessions: Based on clinical response and symptom trajectory
- Neurological monitoring: Cognitive assessment before, during, and after the course
The Time Window That Defines Outcomes
The MDPI Diagnostics 2024 data establishes 200 minutes as the critical threshold — patients treated within this window had dramatically lower DNS risk. In practice, this means:
- Recognition of CO poisoning must happen fast — carbon monoxide detectors are the primary tool
- Pre-hospital 100% oxygen should begin during transport — this buys time but does not replace HBOT
- The emergency department must have a clear protocol for HBOT referral — not as an optional add-on, but as a time-critical pathway for qualifying patients
- The nearest hyperbaric chamber’s contact details should be part of every emergency department’s CO poisoning protocol
Frequently Asked Questions
If I feel fine after CO exposure, do I still need HBOT?
Feeling fine is the most dangerous presentation in CO poisoning. DNS develops in patients who appear to have fully recovered — sometimes weeks after discharge. Clinical guidelines recommend HBOT for any patient with significant CO exposure history, loss of consciousness, or neurological symptoms regardless of how they feel at presentation. The absence of current symptoms does not indicate the absence of ongoing neurological damage.
How quickly does HBOT need to happen?
The research is specific: treatment within 200 minutes of CO exposure is associated with dramatically lower DNS risk. HBOT initiated within 6 hours is standard guidance for qualifying patients. Beyond 24 hours, the acute-phase evidence is weaker — though HBOT is sometimes used for established DNS in a rehabilitation context. Earlier is always better.
Is HBOT safe for pregnant women after CO poisoning?
HBOT is specifically recommended for pregnant patients with CO poisoning — not cautiously, but proactively. The foetus is more susceptible to CO-mediated damage than the mother because foetal haemoglobin binds CO more avidly and foetal tissues are particularly sensitive to hypoxia. The risk of HBOT to the foetus has been studied and is considered acceptable given the alternative: the risk of CO-mediated foetal neurological damage without HBOT is considerably higher.
What if HBOT is not available at my nearest hospital?
Administer 100% oxygen via non-rebreather mask immediately and arrange emergency transfer to the nearest hyperbaric facility. Document the time of CO exposure accurately — this information directly influences treatment decisions. Most major Indian metros have at least one hospital-based hyperbaric unit. In Delhi NCR, Mumbai, Bangalore, Hyderabad, and Chennai, HBOT facilities exist within reasonable emergency transport distance.
How do I know if a family member is developing DNS after CO poisoning?
Watch for these warning signs in the days and weeks following apparent recovery: new difficulty with memory or concentration, uncharacteristic irritability or emotional changes, slowed thinking or speech, unusual fatigue, new incontinence, or any change in personality or behaviour. If any of these emerge, return to emergency care immediately and specifically ask about HBOT for CO-related DNS.
Is HBOT available for CO poisoning treatment in India?
HBOT for CO poisoning is available at hospital-based hyperbaric units in major Indian cities. For a detailed city-by-city guide, visit our or find .
The Damage Is Not Finished When the Exposure Ends
That is the truth about carbon monoxide poisoning that most survivors never fully understand. The gas is gone. The COHb has cleared. The patient seems fine. And the neurological damage cascade is still running.
HBOT interrupts that cascade. It does not do so by replacing the oxygen CO stole — standard oxygen therapy does that. It does so by addressing the downstream injury processes that standard oxygen therapy cannot reach: the oxidative stress, the neuroinflammation, the mitochondrial failure, the perivascular damage.
The evidence on DNS prevention is not ambiguous. The timing window is not wide. And the stakes — cognitive function, personality, memory, independence — are among the highest in medicine.
To understand HBOT’s mechanism of action in full, visit . For neurological condition applications beyond CO poisoning, explore our .
The brain that survived the exposure deserves the treatment that protects what remains.


4 Comments
Comments are closed.


[…] understand the full mechanism of how HBOT fights infection, read our article on carbon monoxide poisoning and HBOT brain protection — which covers HBOT’s anti-inflammatory mechanisms in depth. For the broader conditions […]
[…] visit our HBOT clinics and locations section. You may also find our recently published guide on carbon monoxide poisoning and HBOT useful for understanding how HBOT addresses other acute emergency […]
[…] the full clinical evidence and treatment protocol, see our guide on carbon monoxide poisoning and HBOT brain protection. For the foundational mechanism behind how pressure changes oxygen delivery, visit How HBOT […]
[…] the detailed CO poisoning treatment evidence, see our article on carbon monoxide poisoning and HBOT brain protection. For the foundational mechanism, visit How HBOT […]