

Hyperbaric Oxygen Therapy Benefits for Burn Recovery: What the Science Shows
Burn wounds create three zones. One is already dead. One will heal on its own. The middle zone — the zone of stasis — is the battleground. Hyperbaric oxygen therapy benefits this zone more directly than any other intervention available.

hyperbaric oxygen therapy benefits burns — HBOT burn wound healing recovery zone of stasis
Hyperbaric oxygen therapy benefits burns in a way that standard wound care structurally cannot.
That sentence is worth understanding carefully before everything else. Standard burn wound care is not inadequate — it is excellent at what it does. Dressings preserve moisture. Debridement removes dead tissue. Antibiotics manage infection. But standard care works with the healing process. It cannot restore the oxygen supply that burn tissue needs to initiate that process.
Hyperbaric oxygen therapy restores that supply. Not through a drug or a surgical intervention — through physics. Oxygen dissolved in blood plasma at therapeutic pressure reaches the burn wound margin through diffusion, independent of the damaged circulation that the burn itself destroyed.
The tissue that is alive but dying in the 24 to 48 hours after a burn — the zone of stasis — can be converted to healing tissue. This is not an incremental improvement on standard care. It is a different mechanism entirely, addressing a layer of the problem that standard care cannot reach.
The mechanism is explained fully at How HBOT Works. This article covers the specific benefits for burn recovery — the evidence, the protocol, and what this means for outcomes in India.
Hyperbaric oxygen therapy (HBOT): A treatment in which the patient breathes 100% pure oxygen inside a pressurised chamber at 1.5 to 2.4 times normal atmospheric pressure. Under pressure, oxygen dissolves directly into blood plasma — reaching hypoxic tissue through diffusion without needing functional blood vessels.
Hyperbaric Oxygen Therapy Benefits: Why Burns Create the Zone of Stasis
Every significant burn creates three concentric zones of injury. The innermost zone is dead — the tissue destroyed by direct heat contact. The outermost zone is inflamed but viable, and will heal without specific intervention. Between them sits the zone that determines outcomes.
The zone of stasis is living tissue in a state of progressive oxygen crisis. Microvascular damage has slowed circulation. Oedema has raised interstitial pressure. Inflammatory mediators are consuming oxygen faster than the compromised vessels can deliver it.
Without intervention, this tissue converts to necrosis within 24 to 48 hours. With HBOT, it can survive.
| Zone | Tissue Status | Standard Care Role | HBOT Benefit |
| Zone of Coagulation (centre) | Irreversibly dead — direct thermal destruction | Debridement of necrotic tissue | None — tissue already dead |
| Zone of Stasis (margin) | Alive but dying — hypoxic, inflammatory, progressive necrosis | Dressings and antibiotics limit worsening | PRIMARY BENEFIT — oxygenates, reduces inflammation, rebuilds supply |
| Zone of Hyperaemia (outer) | Viable — increased flow, mild inflammation | Routine wound care sufficient | Accelerates healing; reduces scar risk |
The zone of stasis is where the treatment decision determines whether the burn wound is 5 square centimetres or 15. Whether one graft is needed or three. Whether recovery takes weeks or months. HBOT addresses it directly.
Four Specific Hyperbaric Oxygen Therapy Benefits in Burn Care
Benefit 1 — Oxygenation of Hypoxic Burn Tissue
At 2.0 to 2.4 atmospheres absolute (ATA), oxygen dissolves into blood plasma at concentrations 15 to 20 times higher than at sea level. This plasma-dissolved oxygen reaches the zone of stasis through diffusion — without needing functional capillary flow.
The cells in the zone of stasis are not dead. They are failing because of oxygen deprivation. HBOT delivers what they need to survive. Cellular energy production restores. The death cascade halts. Tissue that would have become necrotic becomes viable.
confirmed that HBOT delivers measurable wound healing improvement specifically by restoring the oxygen gradient that compromised burn tissue cannot generate on its own.
Benefit 2 — Reducing the Inflammatory Cascade
Burns trigger a systemic inflammatory response that consumes oxygen, worsens oedema, and recruits inflammatory cells causing secondary tissue damage beyond the original injury.
HBOT at therapeutic pressure directly reduces this cascade. documented that HBOT reduces neutrophil-endothelium adhesion and reactive oxygen species signalling — limiting the inflammatory second wave that progressively destroys viable tissue in the zone of stasis.
This anti-inflammatory benefit is one of the primary reasons HBOT produces measurably better outcomes in burn wounds compared to standard care alone.
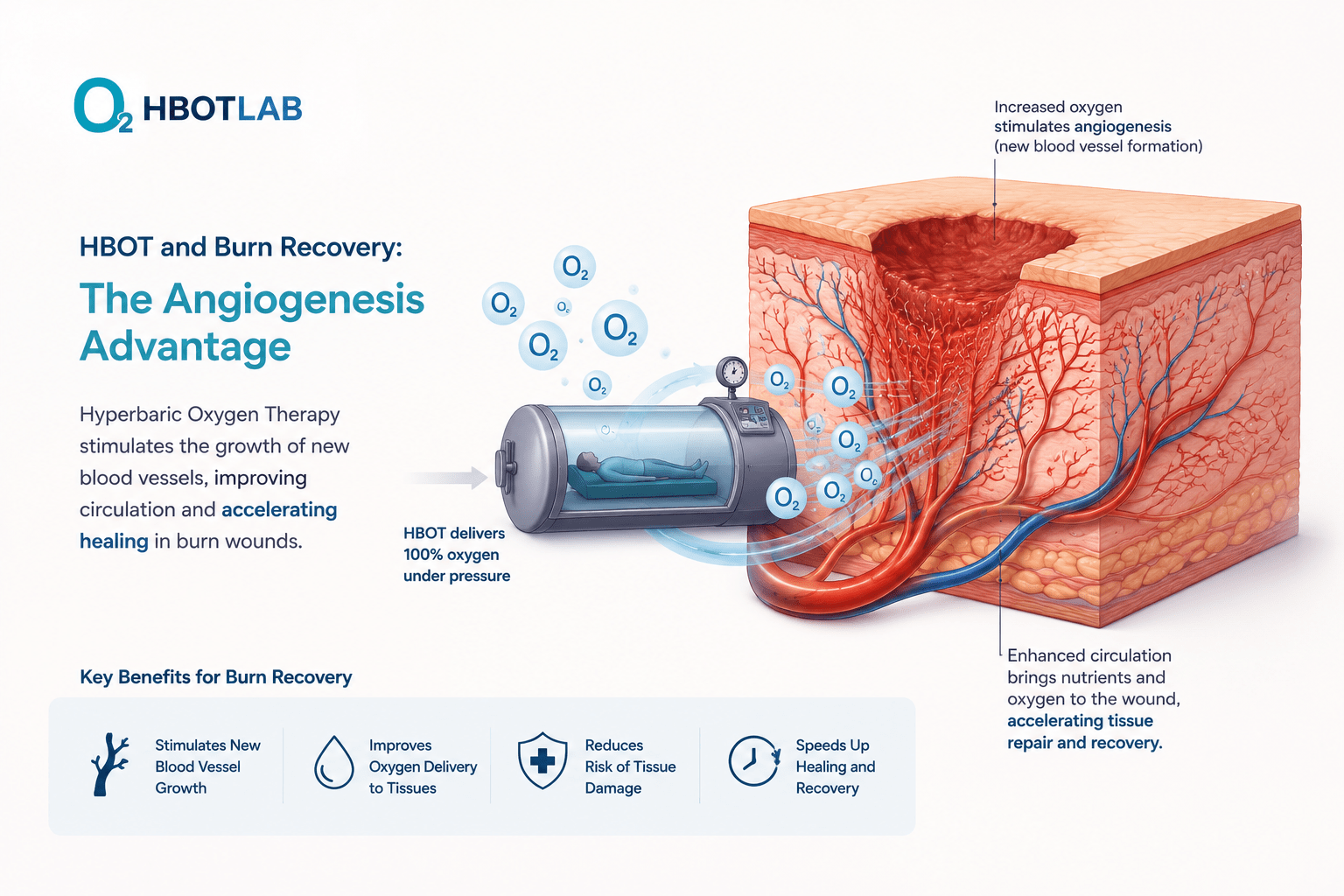
Benefit 3 — Rebuilding the Damaged Microcirculation (Angiogenesis)
Burn injury destroys the microvasculature in and around the wound. Even after the acute phase, this compromised blood supply makes long-term healing difficult and increases wound breakdown risk.
HBOT’s hyperoxic-hypoxic cycle stimulates vascular endothelial growth factor and mobilises vasculogenic stem cells — triggering new capillary growth in the damaged wound bed. documented measurable neovascularisation in hypovascular tissue with HBOT — creating lasting improvement in blood supply that persists long after the treatment course ends.
Benefit 4 — Reducing Infection Risk in Burn Wounds
Burn wounds are highly susceptible to infection. Destroyed skin removes the primary barrier. Hypoxic tissue impairs immune function. HBOT creates a high-oxygen wound environment hostile to anaerobic bacteria and potentiates leukocyte killing of aerobic organisms.
For burns with established or threatened infection, this anti-infective benefit directly reduces mortality risk — burn infection remains the leading cause of burn mortality beyond the acute phase.
hyperbaric oxygen therapy benefits burns — angiogenesis mechanism zone of stasis wound healing
HBOT Benefits Across All Three Phases of Burn Wound Healing
Wound healing proceeds through three overlapping phases. Burns disrupt all three by destroying the oxygen supply each requires. HBOT addresses this disruption at every stage — not only in the acute window.
| Healing Phase | Oxygen Requirement | How Burns Disrupt It | HBOT Benefit |
| Inflammatory (Days 0–4) | O₂ for immune cell killing and bacterial clearance | Hypoxia impairs leukocyte function; infection establishes | Restores tissue O₂ for immune function; anti-infective |
| Proliferative (Days 4–21) | O₂ for fibroblast activity and collagen production | Hypovascular wound bed limits fibroblast function | Plasma oxygenation activates fibroblasts; angiogenesis rebuilds supply |
| Remodelling (Weeks–months) | Sustained O₂ for collagen maturation and scar organisation | Ongoing vascular compromise limits repair quality | Neovascularisation provides lasting supply for quality remodelling |
| FDA Protocol | Acute thermal burns are formally recognised by the US FDA as an HBOT indication. Standard protocol: twice-daily sessions for up to 30 sessions. HBOT is adjunctive to standard burn wound care — debridement, grafting, and infection management remain essential. |
Skin Graft Survival — Where Hyperbaric Oxygen Therapy Benefits Are Clearest
Skin grafting is the primary surgical intervention for serious burns. Whether the graft survives depends directly on the condition of the graft bed — its oxygen level, its vascular supply, and its infection status.
These are precisely the three conditions HBOT addresses. A better-oxygenated, better-vascularised, and cleaner graft bed produces higher graft take rates — reducing failed grafts, repeat surgeries, and prolonged recovery.
A 2024 review published in documented that HBOT significantly improves graft survival by mitigating ischaemia and infection at the graft bed — with comparative data showing reduction in major complications in complex burn cases.
For high-risk burn graft patients — elderly patients, diabetics, extensive burns, burns in poorly vascularised areas — HBOT in the peri-operative period is the evidence-based approach to improving take rates.
Burn Injuries in India — Why These HBOT Benefits Matter Here
India carries one of the highest burn injury burdens globally. Approximately 7 million people suffer serious burns annually — from open flame cooking fires, kerosene stove accidents, electrical burns, and industrial injuries. Burn mortality in India remains significantly higher than international benchmarks.
The hyperbaric oxygen therapy benefits described in this article are not theoretical for Indian patients. They are directly applicable to the most common burn presentation in India — the flame burn from domestic cooking — where zone-of-stasis tissue conversion, graft survival improvement, and infection reduction are all clinically relevant outcomes.
HBOT for burns is available at hospital-based hyperbaric units in Delhi NCR, Mumbai, Bangalore, Hyderabad, and Chennai. Awareness among Indian burn surgeons is growing but remains limited outside major centres.
For HBOT facility locations, see our guides to HBOT in Delhi and HBOT in Bangalore. For session costs, see our HBOT cost guide. For help finding a qualified provider, read our HBOT near me India guide.
For the related hyperbaric oxygen therapy benefits in diabetic wound healing — which shares the ischaemic wound bed mechanism — see our guide on HBOT for diabetic foot wounds.
Frequently Asked Questions
When should HBOT start after a burn injury?
Within 24 to 48 hours of the burn for maximum zone-of-stasis benefit. The zone converts progressively to necrosis within this window. HBOT initiated early preserves tissue that would otherwise be lost. After 48 hours, HBOT continues to provide healing, graft preparation, and anti-infective benefits — but the critical tissue-preservation window has largely closed.
How many HBOT sessions are needed for burns?
The FDA protocol specifies twice-daily sessions for up to 30 sessions for acute thermal burns. Smaller burns in well-vascularised patients may require fewer sessions. Extensive burns in compromised patients — elderly, diabetic, poor peripheral circulation — typically benefit from the full course. Session count is determined by wound response assessed at regular intervals.
Does HBOT replace skin grafting?
No. Grafting remains the primary surgical intervention for significant full-thickness burns. HBOT changes the graft bed conditions — oxygenating it, reducing infection, stimulating vascular growth — to improve take rates. It is a pre- and post-operative adjunct, not a replacement for surgical reconstruction.
Does HBOT help reduce burn scarring?
Evidence for scar quality improvement is emerging. Better oxygenation of the remodelling phase — where collagen maturation and organisation determine scar quality — is associated with more organised collagen deposition and reduced hypertrophic scarring. HBOT does not prevent scarring from serious burns. Reduction in scar severity and improved functional outcomes are the documented goals.
Do hyperbaric oxygen therapy benefits apply to chemical and electrical burns?
Yes — the mechanism is identical. Chemical and electrical burns create the same zone-of-stasis physiology. Electrical burns in particular cause deep tissue injury along the path of current conduction, creating ischaemic zones at depth inaccessible to standard wound care. Plasma-diffusion oxygenation is specifically relevant for deep electrical injury where blood supply has been disrupted along the current path.
Is HBOT available for burn treatment in India?
Yes — at hospital-based hyperbaric units and dedicated wellness HBOT centres in major Indian metros. For a comprehensive guide to finding qualified facilities, see our HBOT near me India buyers guide.
The Zone of Stasis Can Be Won
The hyperbaric oxygen therapy benefits described in this article converge on one clinical outcome: the zone of stasis — the dying tissue that surrounds every serious burn — can be converted to healing tissue rather than lost to progressive necrosis.
This matters enormously for the patient. A smaller final wound means less grafting. Better-prepared graft beds mean higher take rates. Reduced infection means lower mortality. Improved microcirculation means better long-term outcomes.
The therapy exists. The FDA recognises it. The evidence supports it. For Indian burn patients and families — and for the surgeons who treat them — knowing these benefits exist and asking for access to them is the next step.
Zone of stasis tissue that is alive at 24 hours after a burn can still be alive at 48 hours — if it receives the oxygen it needs. HBOT is the only intervention that delivers that oxygen through compromised circulation. The window is real. The benefit is documented.
For the complete mechanism behind hyperbaric oxygen therapy benefits, visit How HBOT Works. For the conditions overview, see our HBOT conditions reference.
Burns define a moment. Recovery defines what comes after. HBOT changes that recovery.



One Comment
Comments are closed.


[…] 6. Can HBOT skin therapy help with scars and wound healing beyond grafting? Yes — HBOT skin therapy for general wound healing and scar management is supported by the same angiogenesis and oxygenation mechanisms. For burn wound healing specifically, see our article on HBOT for burns. […]