
Hyperbaric Oxygen Therapy Before and After: What Radiation Injury Patients Can Expect
The question every radiation injury patient asks before starting HBOT is the same: will I actually see a difference? The honest answer is: yes — if you have the right condition, start at the right time, and complete the full course. Here is exactly what changes, when it changes, and what the evidence shows.
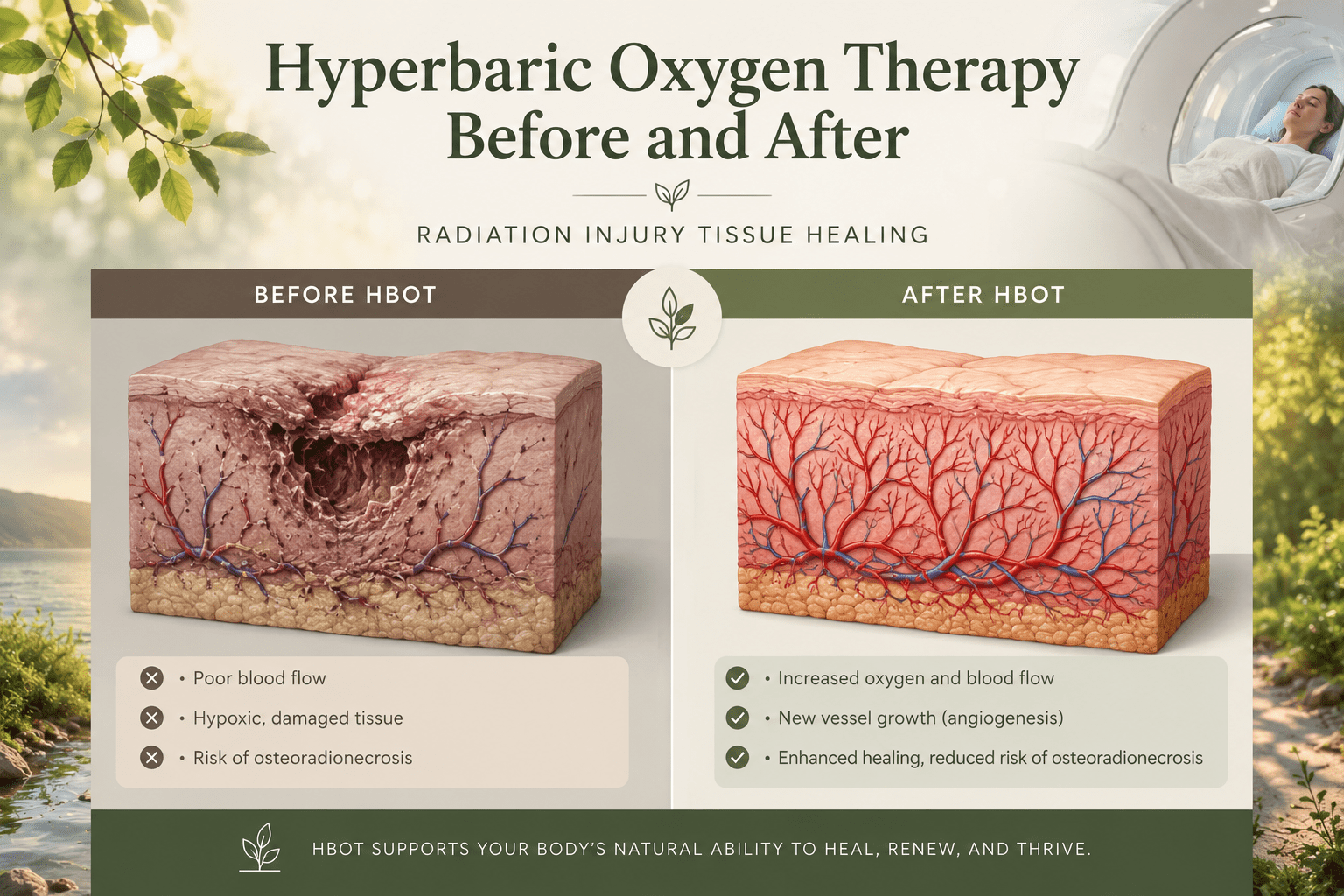
hyperbaric oxygen therapy before and after — radiation injury tissue healing angiogenesis osteoradionecrosis
Hyperbaric oxygen therapy before and after results for radiation injury follow a predictable biological timeline.
Unlike acute emergency conditions — where HBOT produces visible results within the first session — radiation injury recovery is a cumulative process. The angiogenesis that HBOT triggers takes weeks to develop. The new blood vessels that grow in radiation-damaged tissue take the full course of sessions to establish. And the tissue changes that follow — healing of bone, cessation of bleeding, closure of wounds — occur progressively after that.
Understanding this timeline is essential for two reasons. It sets accurate expectations — so patients complete the full course rather than stopping early when early-session results appear modest. And it identifies the patient groups most likely to benefit, so the right candidates start treatment and the wrong candidates are not given false hope.
For the evidence behind why HBOT works for radiation injury, see our guide on HBOT for radiation injury in cancer survivors and our cancer survivor awareness article on HBOT and cancer radiation recovery.
Hyperbaric oxygen therapy before and after (radiation injury context): The biological changes that HBOT produces in radiation-damaged tissue — new blood vessel formation, tissue oxygenation, fibroblast reactivation — occur over a course of 30 to 40 sessions. Visible clinical results follow the biological changes, not the sessions themselves. The full before-and-after transformation in radiation injury takes 3 to 6 months from treatment start to maximum benefit.
Hyperbaric Oxygen Therapy Before Treatment: What Patients Should Do First
The before-and-after outcomes for radiation injury HBOT are significantly influenced by what happens before the first session. These are not optional preparation steps — they directly affect how much benefit the treatment course produces.
Step 1 — Oncologist Clearance
All candidates for HBOT radiation injury treatment must have confirmed remission — or at minimum, a treating oncologist’s assessment that HBOT is appropriate given their current cancer status. This is a non-negotiable pre-treatment step. HBOT is used for radiation injury in cancer survivors, not for patients in active treatment (with specific exceptions, such as ORN prevention before dental extraction in a patient still receiving maintenance therapy).
Step 2 — Comprehensive Assessment at the Hyperbaric Centre
Before the first session, patients undergo a full clinical assessment: wound measurement and photography for baseline documentation, imaging of affected bone if osteoradionecrosis is the indication, pulmonary function assessment, and ear and sinus examination. This baseline is essential for measuring the before-and-after outcome accurately — without it, improvement is subjective rather than documented.
Step 3 — Dental Assessment for Head and Neck Radiation Patients
Patients who have received head and neck radiation and have any dental work planned should have a complete dental assessment before starting HBOT and before any dental extraction. Tooth extraction in irradiated bone without HBOT carries a 10 to 15% risk of osteoradionecrosis. The standard protocol — 20 HBOT sessions before extraction and 10 after — reduces this risk to under 5%.
Step 4 — Establishing Realistic Outcome Expectations
The most important pre-treatment step for patient experience and treatment completion is honest expectation-setting. Radiation injury HBOT does not produce dramatic visible changes in the first two weeks. Patients who understand this complete the course. Those who do not often abandon treatment at session 15 — precisely when the angiogenesis they need is only beginning to develop.
Hyperbaric Oxygen Therapy After Each Session: Week-by-Week Changes
The before-and-after timeline for radiation injury HBOT follows a consistent biological pattern across indication types.
| Timeline | What Is Happening Biologically | What Patients May Notice |
| Sessions 1–10 (Weeks 1–2) | Plasma oxygenation begins — hypoxic tissue receives O₂ for first time. Inflammatory markers reduce. Fibroblast activation begins. | Reduction in pain or discomfort at wound site. Improved general energy in some patients. No visible wound change yet. |
| Sessions 10–20 (Weeks 2–4) | Angiogenesis begins — VEGF triggered, vasculogenic stem cells mobilised. New capillary buds forming in radiation-damaged tissue. | Some patients notice reduced bleeding (proctitis/cystitis). Wound margins may show early granulation tissue. Bone pain may reduce. |
| Sessions 20–30 (Weeks 4–6) | New vessels establishing. Tissue oxygenation sustained. Collagen production increasing. Wound healing cascade activating. | Visible wound improvement in most patients. Bleeding cessation in radiation proctitis common at this stage. Bone healing beginning in ORN. |
| Sessions 30–40 (Weeks 6–8) | Full angiogenesis benefit. Tissue oxygen levels sustained between sessions. Wound remodelling in progress. | Significant wound changes in most responders. Proctitis and cystitis symptoms substantially reduced or resolved in responding patients. |
| 4–12 weeks post-treatment | Angiogenesis continues after course ends — new vessels mature and stabilise. | Maximum benefit often not visible until 4–8 weeks after last session. Bone healing in ORN continues for months post-treatment. |
The most important thing radiation injury patients need to know about HBOT before and after is that the maximum benefit comes after the treatment course ends — not during it. Angiogenesis continues for weeks and months after the last session. Stopping at session 20 because results seem modest is stopping before the transformation has had time to occur.
Before and After by Indication — What the Evidence Shows
Osteoradionecrosis — Bone Healing in Head and Neck Cancer Survivors
documented HBOT outcomes in radiation injury including ORN — showing measurable improvement in bone healing and wound closure in patients who completed the full treatment course. The before-and-after distinction for ORN is typically visible at the 3-month post-treatment assessment: bone exposure reducing, granulation tissue forming over previously exposed bone, pain reduction documented on standardised scales.
For ORN that has progressed to the point of requiring surgical resection, HBOT is used both before surgery (to improve the condition of the resection site) and after (to support healing of the reconstructed area). The before-and-after comparison in these cases is measured in terms of surgical success rate and healing timeline rather than wound appearance alone.
Radiation Proctitis — Bleeding Cessation and Symptom Resolution
The before-and-after transformation for radiation proctitis is among the most clearly measurable in the radiation injury indication. Rectal bleeding — the primary symptom — is objectively quantifiable at baseline and at each assessment point. Multiple clinical series document cessation or significant reduction in bleeding in 70 to 85% of patients who complete a 30 to 40 session course.
reviewed the radiation proctitis evidence confirming that HBOT’s angiogenic mechanism — rebuilding the mucosal blood supply that radiation destroyed — is the mechanism behind the bleeding cessation seen in responding patients. The before-and-after change is not symptomatic management. It is structural repair of the tissue causing the symptom.
Radiation Cystitis — Haematuria Resolution
For radiation cystitis — blood in the urine caused by radiation damage to the bladder mucosa — the before-and-after outcome follows the same pattern as proctitis. Haematuria reduction begins typically in the third week of treatment and continues to improve after the course ends as the newly formed mucosal vasculature matures.
Soft Tissue Wounds — Closure and Healing
Non-healing radiation wounds that have been open for months or years show the most dramatic before-and-after visual change with HBOT. Wound measurements at baseline versus session 20 versus session 40 versus 8 weeks post-treatment typically show progressive reduction in wound area and depth, with granulation tissue formation that standard wound care alone could not produce in the same hypovascular tissue environment.
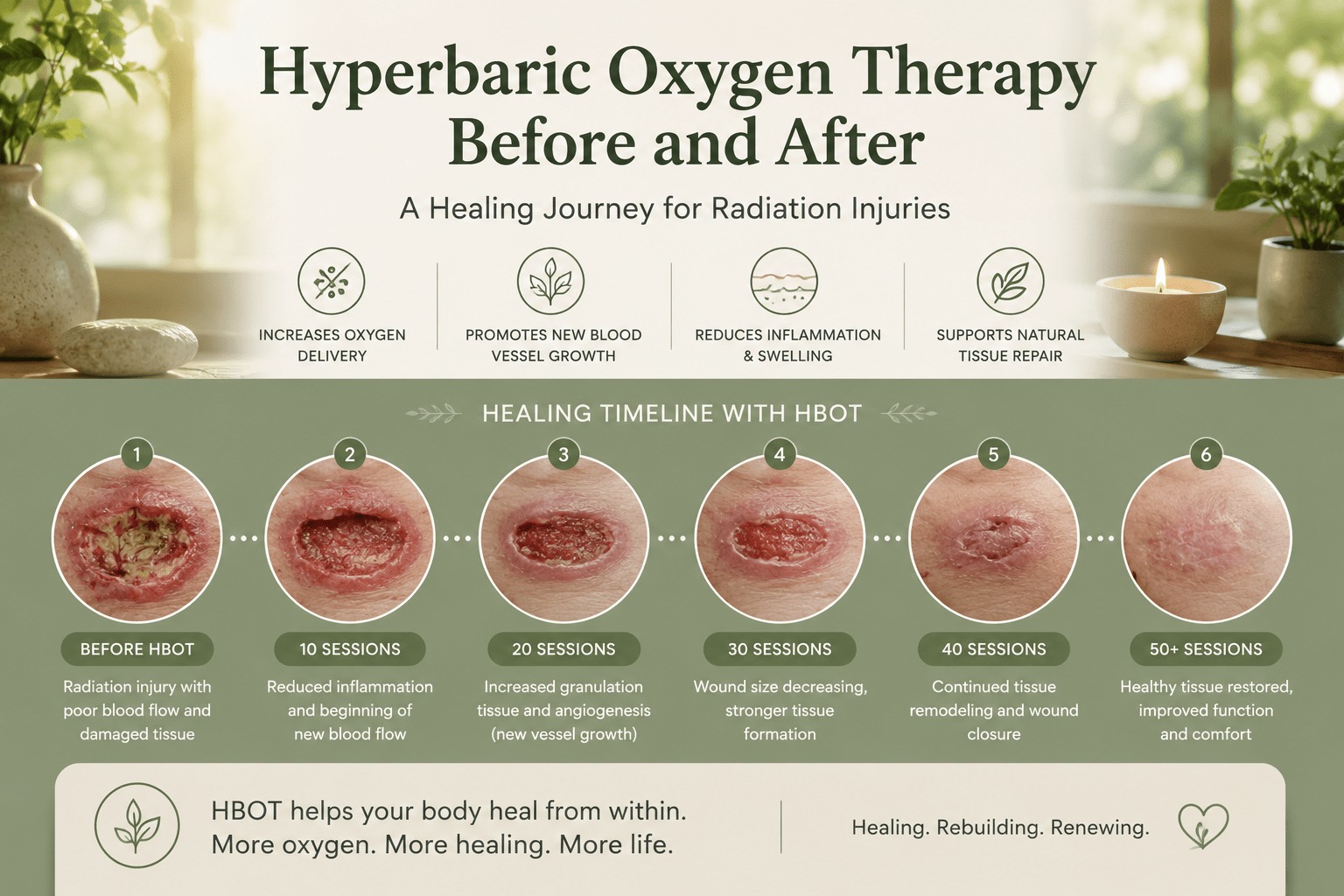
hyperbaric oxygen therapy before and after — radiation wound timeline progress healing angiogenesis
Who Does Not Respond — Understanding the Limits of Before and After
Honest before-and-after outcomes require honest acknowledgement of non-response. Not all radiation injury patients respond to HBOT, and setting accurate expectations includes explaining who is less likely to benefit.
- Established bone death (stage III ORN) without surgery: HBOT alone cannot reverse extensive bone necrosis. Surgical resection followed by HBOT-supported reconstruction is the standard for advanced ORN.
- Very long-standing wounds (>10 years): the fibrotic changes in very chronic radiation wounds are less reversible than in wounds of 1 to 5 years duration.
- Active smoking during treatment: smoking significantly impairs angiogenesis and reduces HBOT efficacy. Patients who cannot stop smoking during the treatment course should be counselled that results will be substantially reduced.
- Incomplete course: patients who stop before session 30 rarely achieve the full angiogenesis benefit. Partial courses produce partial results.
| Realistic Expectation | 70–80% of radiation injury patients who complete a full 30–40 session course show clinically significant improvement. 20–30% do not respond adequately. The responders typically show maximum benefit 4–8 weeks after their last session. Patients assessed only at session 20 and declared non-responders are frequently those who would have responded with the full course. |
Accessing HBOT for Radiation Injury in India — Practical Before You Start
India’s cancer treatment burden means a large and growing population of radiation injury patients. The practical before-you-start questions for Indian cancer survivors considering HBOT are access, cost, and insurance.
For HBOT facilities near you, see our guides to HBOT in Delhi and HBOT in Bangalore. For comprehensive national access guidance, visit our HBOT near me India guide.
For cost information, see our guides to HBOT cost in Mumbai and HBOT therapy cost in Delhi. For insurance coverage guidance, see our HBOT insurance India guide.
Frequently Asked Questions
How soon after finishing radiation therapy can I start HBOT?
Late radiation injury can present months to years after radiation therapy ends — there is no upper time limit on when HBOT becomes relevant. For pre-operative HBOT (before surgery in irradiated tissue), the standard is to begin as soon as the need is identified, regardless of when radiation was received. For established late radiation injury, earlier treatment produces better outcomes than waiting — the longer the tissue remains hypoxic, the more fibrotic and less responsive it becomes.
Will HBOT before and after radiation injury improve my quality of life?
Yes — in responding patients, quality of life improvement is the primary patient-reported outcome across all radiation injury indications. Cessation of rectal bleeding, resolution of bladder haematuria, healing of non-healing wounds, and reduction in bone pain all translate directly into measurable quality of life improvement. Multiple clinical series use validated quality of life instruments to document this — the improvements are not subjective impressions but measured outcomes.
Can I continue my cancer medications during HBOT?
Most cancer maintenance medications are compatible with HBOT. The key exception is bleomycin — a chemotherapy agent with a specific HBOT interaction that can cause pulmonary toxicity. Any patient on or recently off bleomycin should discuss this with their oncologist and the hyperbaric physician before starting. All other standard cancer medications, hormone therapies, and supportive care medications are generally compatible with HBOT.
What should I bring to my first HBOT session?
- Complete treatment history including radiation dose records and treatment fields if available
- Current medications list
- Any recent imaging (MRI, CT, bone scan) of the affected area
- Wound photographs if available — these become the before baseline for comparison
- 100% cotton clothing — synthetic materials are not permitted in the chamber
- Oncologist clearance letter confirming current remission status
The After Is Worth the Before
Radiation injury patients often arrive at HBOT after years of managing complications that standard medicine has told them are permanent. Non-healing wounds. Ongoing bleeding. Bone that will not heal. They have tried other treatments. They have been told this is simply the price of surviving cancer.
The hyperbaric oxygen therapy before and after data says something different. In 70 to 80% of patients who complete the full course, the tissue that radiation permanently damaged becomes tissue that heals. The bone that would not heal begins to knit. The bleeding that continued for years stops. The wound that has been open since the mastectomy closes.
The timeline is real. The mechanism is documented. The results are measurable. For Indian cancer survivors — the conversation to have with your oncologist is not whether HBOT might help. It is whether the referral can be made before more tissue is lost to the irreversible fibrosis that chronic hypoxia produces.
The radiation injury patients most likely to see dramatic before-and-after change are those with documented late radiation damage — wounds, bleeding, bone exposure — who have not yet developed end-stage fibrosis. For these patients, the angiogenesis that HBOT triggers does not just manage symptoms. It rebuilds the infrastructure that radiation destroyed. The new blood vessels are real. The tissue healing that follows is measurable.
For the full radiation injury primary evidence, see our guide on HBOT for radiation injury in cancer survivors. For all 14 indication uses of HBOT, see our HBOT uses guide. For the mechanism behind how pressure delivers oxygen to damaged tissue, visit How HBOT Works.
The tissue radiation damaged is not beyond reach. The question is whether the course is completed.




