

Cancer Treatment Ended. The Damage Did Not. How HBOT Heals Radiation Injury
Radiation does not simply damage tissue and stop. It permanently alters the blood supply — creating a wound that cannot heal without intervention. HBOT restores what radiation destroyed.
HBOT radiation injury cancer survivors — hyperbaric oxygen therapy late radiation tissue damage

You won. That is not a small thing.
Cancer treatment is one of the hardest things a person goes through. The surgery, the chemotherapy, the radiation — the months of fighting something that lived inside your body. And then the scan came back clear. The oncologist used the word remission. You crossed a threshold that many do not.
And then something else appeared. Not the cancer — that is gone. Something the radiation left behind. A wound that will not close. Pain in the jaw that no dentist can explain. A bowel that has never quite recovered. Tissue that looks healed from the outside and will not heal on the inside.
This is late radiation tissue injury. It is chronic, progressive, and deeply misunderstood — even by patients who have been living with it for years. It is not a recurrence. It is not a complication of poor surgical technique. It is a biological consequence of radiation that standard wound care was not designed to address.
HBOT was. This article explains what radiation does to tissue at the biological level, why that damage persists and progresses years after treatment, and how HBOT addresses the mechanism that everything else leaves untouched.
Editorial commitment: Every claim in this article is backed by peer-reviewed research. HBOT is framed as adjunctive supportive care — not as a cure for cancer, not as a replacement for oncological treatment. If you are in active cancer treatment, please consult your oncologist before beginning HBOT.
What Radiation Does to Tissue — The Long-Term Biology
Radiation therapy works by damaging the DNA of rapidly dividing cells — the cancer cells that need to be destroyed. It is effective. It saves lives. But radiation does not discriminate perfectly between cancer cells and the healthy tissue in the treatment field.
The short-term damage is expected and manageable: inflammation, skin reactions, temporary bowel or bladder changes. These resolve. What does not always resolve is the damage to the blood vessels in the irradiated tissue.
The Three-Part Problem: Hypovascular, Hypoxic, Hypocellular
Radiation permanently damages the small blood vessels — capillaries and arterioles — within the treatment field. Over months and years after treatment ends, these damaged vessels undergo progressive fibrosis and obliteration. Less blood reaches the tissue. Less oxygen arrives. Fewer cells can survive and divide.
The result is what hyperbaric medicine terms the three-H environment: hypovascular (reduced blood supply), hypoxic (oxygen-deprived), and hypocellular (reduced viable cell population). This environment makes normal wound healing biologically impossible.
As documented by in their review of HBOT and wound healing: the hypovascular, hypoxic, hypocellular environment of radiation-damaged tissue is precisely the context in which HBOT’s mechanism — delivering high-concentration dissolved oxygen through plasma — is most directly applicable.
| Tissue Change After Radiation | Timeline | Clinical Consequence |
|---|---|---|
| Acute inflammation and oedema | During and immediately after treatment | Manageable — resolves with standard care |
| Small vessel endothelial damage | Begins during treatment; progressive | Reduced circulation to irradiated field — permanent |
| Vascular fibrosis and obliteration | Months to years after treatment | Progressive ischaemia — worsens over time without intervention |
| Tissue hypoxia | Develops as vascular damage accumulates | Healing cascade cannot initiate — wounds stall or worsen |
| Fibroblast depletion | Parallel to vascular damage | Collagen production impaired — structural repair fails |
| Osteonecrosis (bone in field) | Years after treatment — often triggered by dental procedure | Jaw bone cannot repair — osteoradionecrosis develops |
Radiation injury does not plateau. Without treatment, the three-H environment progresses — more fibrosis, less circulation, deeper hypoxia. The tissue that appeared stable may be moving slowly toward breakdown.
Why Standard Wound Care Cannot Heal Radiation-Damaged Tissue
Standard wound care assumes a baseline of functional tissue biology. Dressings maintain a moist wound environment to support the healing cascade. Debridement removes barriers to healing. Antibiotics address infection. Nutritional support provides the building blocks for repair.
All of these interventions require the wound to have a functional blood supply and an oxygenated tissue environment. They are inputs to a biological process that must already have the capacity to function.
Irradiated tissue does not have that capacity. It is not a wound that is failing to use available resources. It is a wound in a biological environment where the resources — oxygen, viable cells, vascular infrastructure — have been permanently reduced by the radiation itself.
Applying standard wound care to radiation-damaged tissue is providing inputs to a process that cannot receive them. The dressing changes, the debridement, the careful nursing — all of it is correct technique applied to a context for which it was not designed.
HBOT is designed for this context.
How HBOT Reverses Radiation Injury — The Biological Mechanisms
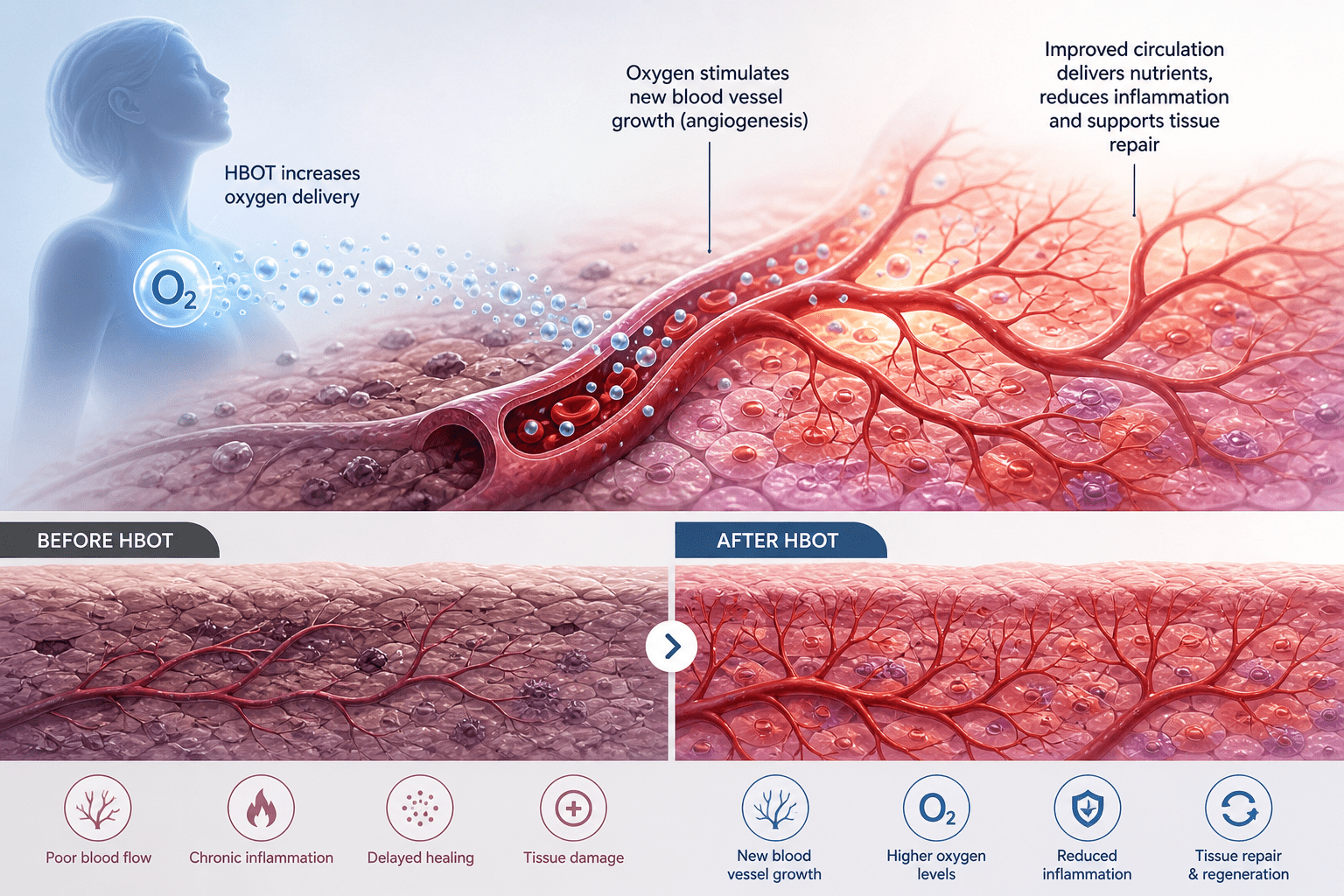
Mechanism 1 — Plasma Oxygenation of Chronically Hypoxic Tissue
At 2.0–2.4 ATA, oxygen dissolves into blood plasma at concentrations 15–20 times higher than at normal atmospheric pressure. This plasma-dissolved oxygen reaches tissue through diffusion — without needing functional small vessel circulation. In a radiation field where capillaries have been obliterated, plasma diffusion is the only oxygenation pathway that still works.
Each HBOT session restores oxygen tension in the irradiated tissue to levels the healing cascade requires. The effect is temporary — oxygen tension returns toward baseline between sessions. But the biological processes that oxygen triggers continue to build between sessions.
Mechanism 2 — Angiogenesis: Rebuilding the Blood Supply
This is HBOT’s most significant long-term contribution to radiation injury healing. The hyperoxic-hypoxic cycle — high oxygen tension during sessions, return to relative hypoxia between sessions — creates the precise signalling environment that stimulates new blood vessel growth.
As documented by , HBOT stimulates vasculogenic stem cell mobilisation and differentiation — the cellular mechanism that produces new capillary networks in previously hypovascular tissue. Over 20 to 40 sessions, measurable neovascularisation occurs in the irradiated field. The blood supply that radiation destroyed begins, gradually, to be rebuilt.
The landmark study by confirmed in a rat model that HBOT reverses radiation-induced pro-fibrotic and oxidative stress responses — demonstrating that the three-H environment itself can be partially reversed, not just managed.
Mechanism 3 — Fibroblast Activation and Collagen Repair
Fibroblasts — the cells responsible for producing collagen and driving the structural repair phase of wound healing — are depleted in irradiated tissue. They cannot function adequately in hypoxic environments. HBOT restores the oxygen gradient that fibroblast activity requires, reactivating the collagen synthesis that radiation has suppressed.
The result is progressive structural repair: new collagen is laid down, wound tensile strength increases, and the tissue gradually regains the architecture that radiation disrupted.
Mechanism 4 — Reducing Radiation-Induced Fibrosis
Radiation injury drives progressive fibrosis through chronic oxidative stress and inflammatory signalling. documented that HBOT reduces this pro-fibrotic response at the molecular level — reducing TGF-beta signalling and inflammatory cytokines in irradiated tissue. Less fibrosis means more functional tissue, less pain, and better healing capacity.
HBOT radiation injury — angiogenesis mechanism hyperbaric oxygen cancer survivor healing
Which Radiation Injuries Respond to HBOT
HBOT for radiation injury is not a single indication. It is a spectrum of conditions sharing the same underlying biology — the three-H environment — in different anatomical locations.
Osteoradionecrosis of the Jaw (ORN)
The most common and distressing form of radiation bone injury. Jaw bone in the radiation field loses its blood supply progressively. Triggered or accelerated by dental procedures — extractions, implants — in the irradiated jaw, ORN presents as exposed bone that will not heal, persistent pain, and difficulty eating.
HBOT is recommended by both the UHMS and the European Committee for Hyperbaric Medicine (ECHM) as standard care for established ORN — and for prevention in high-risk patients undergoing necessary dental procedures post-radiation. The standard protocol is 20 sessions before the dental procedure and 10 after, in addition to the full course for established disease. confirmed measurable healing outcomes with HBOT in radiation injury cases.
Radiation Cystitis
Persistent bladder inflammation, haematuria (blood in urine), and urinary dysfunction following pelvic radiation for prostate, cervical, or bladder cancers. The bladder wall becomes hypovascular and prone to bleeding from fragile new vessels growing into damaged tissue.
HBOT promotes stable, functional neovascularisation of the bladder wall, reducing haematuria and improving bladder capacity. Typically 40 sessions at 2.0–2.4 ATA. Response rates in clinical series are consistently positive.
Radiation Proctitis
Chronic rectal bleeding, urgency, and pain following pelvic radiation. The same hypovascular mechanism as radiation cystitis — progressive ischaemia of the bowel wall, fragile new vessel formation, and impaired mucosal integrity.
The 2023 Cochrane systematic review on HBOT for late radiation tissue injury () found consistent evidence supporting HBOT for both radiation cystitis and radiation proctitis — with an evidence base built across multiple controlled studies.
Soft Tissue Radiation Necrosis
Necrosis in soft tissue within the radiation field — breast, head and neck, chest wall. The tissue cannot heal because it lacks the blood supply and cellular architecture to support repair. HBOT provides the oxygen and angiogenic stimulus that allows healing to proceed.
Radiation Necrosis of the Brain
A late complication of brain radiation therapy — localised necrosis in the irradiated brain region that can cause progressive neurological symptoms. HBOT’s ability to oxygenate hypoxic neural tissue and reduce oedema has produced clinical improvement in documented cases, though this remains an area where evidence is building.
| Cochrane 2023 | The 2023 Cochrane Database systematic review of HBOT for late radiation tissue injury concluded that HBOT is associated with positive outcomes for osteoradionecrosis, radiation cystitis, and radiation proctitis — based on evidence across controlled trials. The review appropriately noted that further high-quality RCTs are warranted for emerging applications. |
What HBOT for Radiation Injury Looks Like — Protocol and Expectations
Standard Protocol Parameters
- Pressure: 2.0 to 2.4 ATA
- Session duration: 90 minutes of oxygen breathing
- Course length: 30 to 60 sessions depending on indication and severity
- Frequency: Once daily, five days per week
- ORN prevention: 20 pre-procedure + 10 post-procedure sessions
- Established ORN: 30 sessions minimum; 60 for severe cases
- Radiation cystitis / proctitis: 40 sessions standard
What to Expect — Realistic Timeline
HBOT for radiation injury is not a rapid intervention. The angiogenesis and fibroblast reactivation that drive long-term healing are cumulative biological processes. Most patients begin to notice improvement in symptoms — reduced pain, improved wound appearance, decreased bleeding in cystitis — after 20 to 30 sessions.
The full biological effect continues for weeks to months after the course ends, as the new blood vessels mature and the collagen remodelling phase progresses. Assessment at 3 months post-completion gives the most accurate picture of treatment outcome.
Not every patient achieves complete healing. For some, HBOT arrests progression and provides significant symptom relief without complete resolution. For others — particularly those treated early, before fibrosis becomes advanced — complete healing is achievable.
Radiation Injury and HBOT in India — What Cancer Survivors Need to Know
India has one of the largest cancer burdens in the world — with approximately 1.5 million new cases diagnosed annually. Head and neck cancers, cervical cancers, and breast cancers — all among the most common in India — are frequently treated with radiation therapy. The consequence is a growing population of cancer survivors living with late radiation tissue injury.
Awareness of HBOT as a treatment option for radiation injury among Indian oncologists and patients remains low. Many patients endure osteoradionecrosis, radiation cystitis, or chronic radiation wounds for years without knowing that an evidence-backed treatment exists.
HBOT for radiation injury is available at hospital-based hyperbaric units in Delhi NCR, Mumbai, Bangalore, Hyderabad, and Chennai. Session costs typically range from Rs. 4,000 to Rs. 8,000. A full course of 40 sessions represents a significant but often transformative investment in quality of life for cancer survivors managing chronic radiation damage.
For HBOT availability and costs in India, see our guides to , , and .
Frequently Asked Questions
1. Can HBOT be used during active cancer treatment?
2. How long after radiation therapy can HBOT be started for radiation injury?
3. Is HBOT safe for cancer survivors?
4. Does HBOT work for osteoradionecrosis of the jaw?
5. How many HBOT sessions are needed for radiation injury?
6. Will insurance cover HBOT for radiation injury in India?
You Survived. Your Tissue Can Recover Too.
The damage radiation left behind is real. It is not in your head. It is not an inevitable permanent consequence you must simply accept. It is a biological wound in a biological environment — and biology can be changed.
HBOT does not undo radiation. It does not reverse every consequence of cancer treatment. But it addresses the specific mechanism that standard care cannot — the permanent reduction in blood supply and oxygen availability that makes radiation wounds different from every other kind of wound.
For osteoradionecrosis, radiation cystitis, radiation proctitis, and soft tissue radiation necrosis, the evidence base is consistent and clinically meaningful. The Cochrane review exists. The UHMS guidance is clear. The mechanism is understood.
You fought through treatment. This is worth fighting for too.
For the complete evidence base on HBOT and cancer support, explore our section. To understand the full mechanism of HBOT, visit .
The cancer is gone. The damage that treatment left does not have to be permanent.
Explore the HBOTLAB Knowledge Centre →



3 Comments
Comments are closed.


[…] For the related evidence on HBOT skin therapy in diabetic wounds — which shares the ischaemic wound bed mechanism — see our detailed guide on HBOT for diabetic foot wounds. For radiation injury healing, see our article on HBOT for radiation injury. […]
[…] the primary radiation injury evidence and treatment protocol, see our guide on HBOT for radiation injury in cancer survivors. For the mechanism behind how HBOT oxygenates hypovascular tissue, visit How HBOT […]
[…] the evidence behind why HBOT works for radiation injury, see our guide on HBOT for radiation injury in cancer survivors and our cancer survivor awareness article on HBOT and cancer radiation […]