
How Many Hyperbaric Oxygen Therapy Sessions Does Osteomyelitis Require — and Why
Patients ask how many sessions. The right answer is not a number. It is an explanation of what each phase of the protocol is doing inside the bone — and why stopping early means stopping before the therapy has worked.
hyperbaric oxygen therapy how many sessions — osteomyelitis protocol phases 30 40 bone infection
Hyperbaric oxygen therapy how many sessions are needed for osteomyelitis? The standard answer is 30 to 40 — but that number only makes sense when you understand what each phase of the protocol is achieving.
Osteomyelitis is one of the longer HBOT indications. Most conditions are treated in 10 to 20 sessions. Bone infection requires 30 to 40 because the mechanism that produces the lasting benefit — angiogenesis, the growth of new blood vessels in hypovascular bone — takes time to establish, and because the antibiotic potentiation benefit it enables needs to be sustained throughout the full course of concurrent antibiotic therapy.
Patients who are told ’30 to 40 sessions’ without explanation frequently stop at session 15 or 20, when they are feeling better but before the angiogenesis that will prevent recurrence has established. Understanding what is happening at each stage of the protocol is the most important factor in completing the course.
For the evidence on why HBOT works for osteomyelitis, see our guide on HBOT for refractory osteomyelitis and our patient decision article on is HBOT good for bone infections.
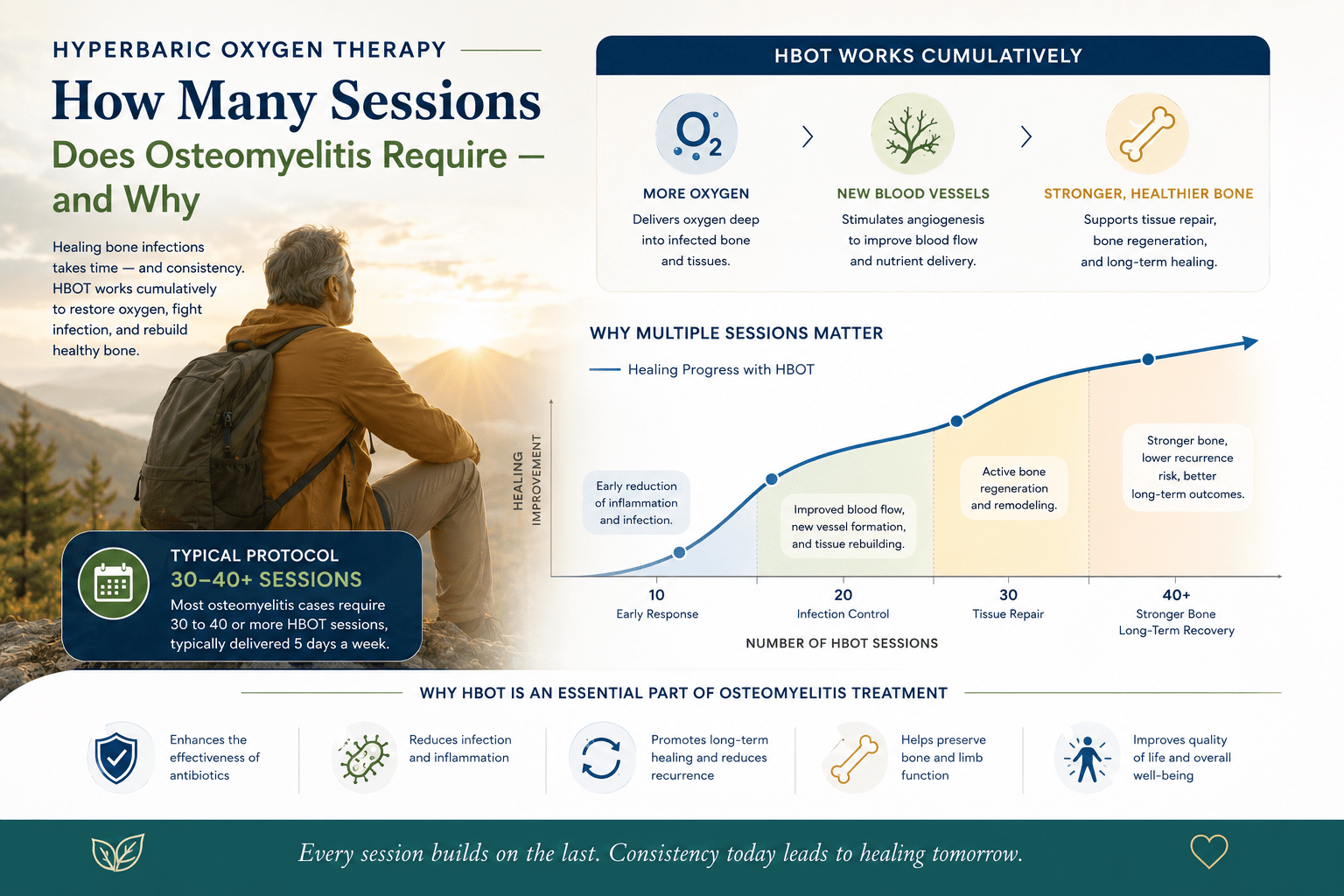
Why osteomyelitis needs more sessions than most indications: Most HBOT indications require oxygen delivery for acute tissue rescue — burns, DCS, CO poisoning. Osteomyelitis requires oxygen delivery for a sustained period to rebuild the chronic hypovascular environment that allowed the infection to become refractory. Angiogenesis — new vessel growth — takes weeks to establish. Sessions 1–10 create the conditions. Sessions 10–30 build the new vessels. Sessions 30–40 allow them to mature.
How Many Sessions Does Hyperbaric Oxygen Therapy Need — The Three Phases
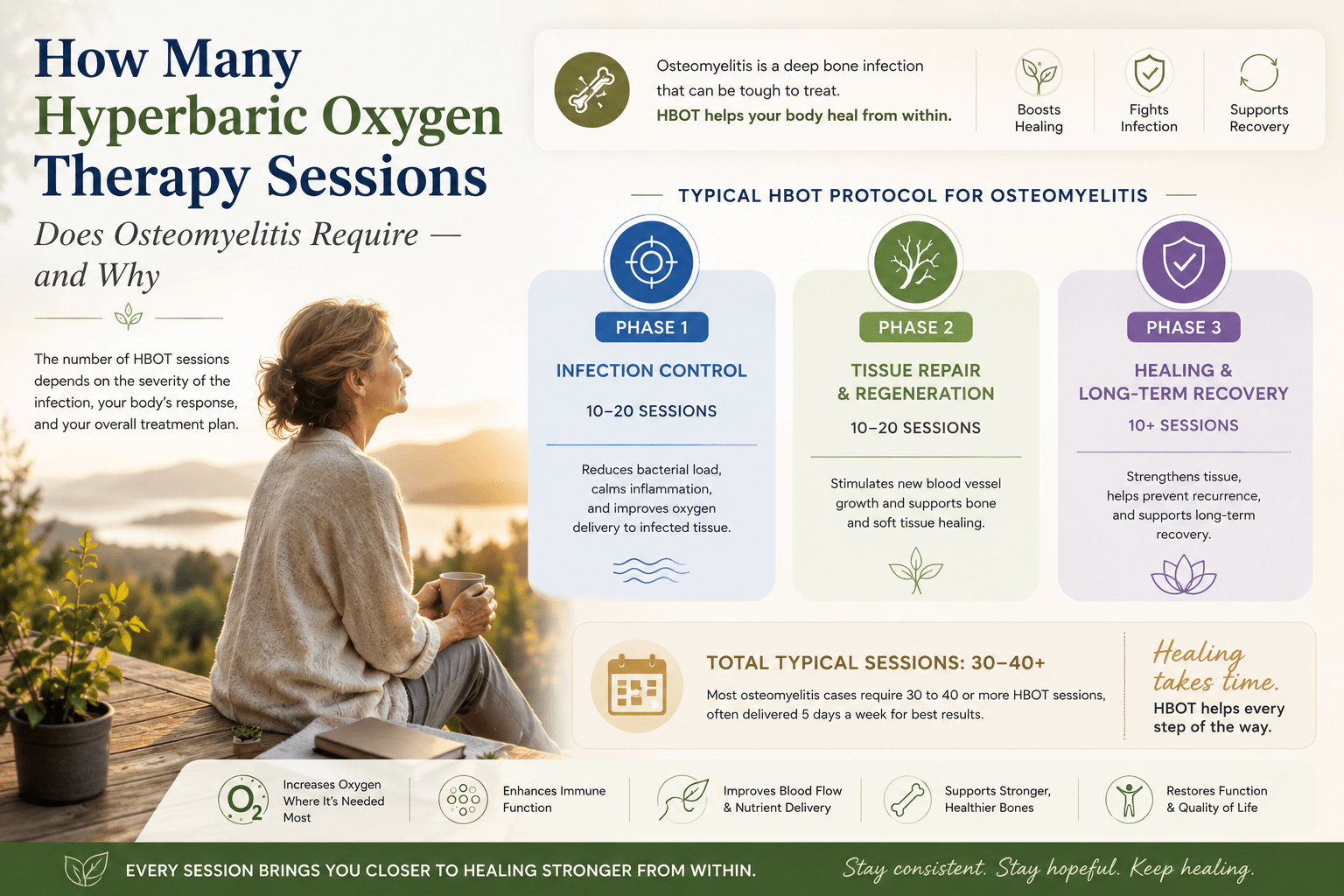
The 30 to 40 session protocol for osteomyelitis is not an arbitrary number. It maps to three distinct biological phases, each of which contributes a different therapeutic benefit.
| Phase | Sessions | Primary Biological Goal | What Patients May Notice |
| Phase 1 Antibiotic Potentiation | Sessions 1–10 (Weeks 1–2) | Tissue O₂ raised above 30 mmHg threshold — aminoglycosides become bactericidal in bone tissue for first time | Possible reduction in systemic infection signs (CRP, fever, WBC). Local pain may reduce. No visible bone change yet. |
| Phase 2 Angiogenesis Initiation | Sessions 10–25 (Weeks 2–5) | VEGF stimulated; vasculogenic stem cells mobilised; new capillary buds forming in hypovascular bone | Continued symptom improvement. Imaging at mid-course may show early periosteal reaction in responding patients. |
| Phase 3 Vascular Maturation | Sessions 25–40 (Weeks 5–8) | New vessels establish and mature; bone tissue oxygenation self-sustaining; cavity healing in post-sequestrectomy cases | Most visible clinical improvement. Wound healing in associated soft tissue. Bone healing on imaging in ORN/osteomyelitis cavity. |
| Post-Treatment Consolidation | 4–12 weeks after last session | Angiogenesis continues independently; new vessels mature; antibiotic course completes its work in now-oxygenated tissue | Maximum benefit often seen 4–8 weeks after last session — not at session 40 itself. |
Session 20 is the most dangerous moment in an osteomyelitis HBOT course. The patient feels better. The infection is responding. The temptation to stop is strongest. But the angiogenesis that will prevent recurrence is only halfway established. Stopping at session 20 means losing the Phase 3 benefit entirely.
Why the Protocol Length Varies — Factors That Change the Session Count
The 30 to 40 session range is a guideline. The actual session count for any individual patient depends on several clinical variables that the treating team assesses at each mid-course review.
Factors That May Require More Sessions (up to 40)
- Diabetic osteomyelitis with peripheral vascular disease — impaired baseline vascularity means angiogenesis takes longer to establish in already-compromised bone
- Post-sequestrectomy cavities — large bone cavities following dead bone removal require extended angiogenesis to support cavity healing
- Multi-site or extensive bone involvement — osteomyelitis affecting multiple bones or a large segment requires sustained treatment to rebuild vascularity throughout the affected area
- Previous radiation to the affected bone — radiation-damaged bone has reduced angiogenic capacity; the hyperoxic-hypoxic stimulus needs more repetitions to establish new vessel growth
- Chronic presentation (>5 years) — very long-standing osteomyelitis with established fibrosis requires the full 40 sessions for maximum angiogenesis benefit
Factors That May Allow Fewer Sessions (down to 25–30)
- Acute-on-chronic presentation with good baseline vascularity — adequate blood supply means angiogenesis establishes faster
- Excellent clinical and imaging response at mid-course review — a patient at session 20 with documented bone healing may achieve the required outcome with 30 total sessions
- Localised infection without extensive bone necrosis — less tissue to revascularise means the threshold is reached faster
What Happens at Each HBOT Session — Inside the Bone
Each 90-minute session at 2.0 to 2.4 ATA contributes to the cumulative biological changes that build across the protocol. Understanding what happens at the session level explains why consistency matters as much as total session count.
During Each Session
Plasma oxygen concentration rises to 15–20 times normal atmospheric levels. This oxygen dissolves into blood plasma and diffuses into the hypovascular bone tissue — reaching areas where the blood vessels destroyed by chronic infection cannot deliver it. Tissue oxygen tension in infected bone rises from near-zero to 200+ mmHg during the session.
At these oxygen concentrations, aminoglycoside antibiotics achieve their full bactericidal mechanism. The immune cells in the infected bone regain their killing capacity. Clostridial and Staphylococcal biofilms are disrupted by reactive oxygen species. The infection — which had been stable or progressing despite antibiotic therapy — begins responding. documented this direct potentiation effect — confirming that HBOT and antibiotics are complementary mechanisms, not alternatives.
Between Sessions
Tissue oxygen levels do not return immediately to pre-treatment baseline between sessions. Studies document persistent elevation of bone tissue oxygen tension for 6–8 hours after each session — sustaining the antibiotic potentiation benefit through most of the inter-session interval in a twice-daily protocol.
More importantly, the angiogenic signalling triggered by each session’s hyperoxic-hypoxic cycle — the elevation during the session followed by the relative hypoxia between sessions — accumulates across the course. documented the vasculogenic stem cell mobilisation that drives this angiogenesis — confirming that the benefit builds cumulatively across the protocol rather than resetting between sessions.
hyperbaric oxygen therapy how many sessions — bone angiogenesis cumulative effect osteomyelitis protocol
The Mid-Course Review — When Assessment Guides the Remaining Count
Standard osteomyelitis HBOT protocol includes a formal mid-course review at session 20 to 25. This review assesses clinical response, imaging changes, and inflammatory marker trends — and determines whether the full 40-session course is indicated or whether the target can be achieved with fewer sessions.
What the Mid-Course Review Assesses
- Inflammatory markers — CRP, ESR, white cell count trend
- Wound status — soft tissue healing in any associated wound or post-surgical site
- Imaging — X-ray or MRI for periosteal reaction, cavity filling, bone density change
- Symptom trajectory — pain, function, systemic signs of infection
- Antibiotic response — clinical assessment from the infectious disease team
| What ‘Responding’ Means at Session 20 | A responding patient at session 20 shows: CRP trending downward from baseline; soft tissue wound (if present) showing granulation; imaging with periosteal reaction or early cavity fill; reduced local pain. A non-responding patient at session 20 warrants reassessment of antibiotic selection, surgical adequacy, and patient compliance with concurrent treatment — before deciding to extend or discontinue HBOT. |
How Many Sessions for Diabetic Osteomyelitis — India’s Most Common Presentation
Diabetic osteomyelitis — typically of the foot, following a diabetic ulcer that has tracked to bone — is the most common osteomyelitis presentation in Indian hyperbaric centres. The session count for diabetic osteomyelitis generally follows the upper end of the range: 35 to 40 sessions.
The reasons are the same as for all diabetic bone complications: peripheral vascular disease has already impaired bone vascularity before infection establishes. Angiogenesis in an already-compromised vascular bed requires more repetitions of the hyperoxic-hypoxic cycle to establish new vessel growth. And the concurrent diabetic wound that typically accompanies foot osteomyelitis often needs the full course to achieve healing as well.
For the diabetic foot wound healing evidence, see our guides on HBOT for diabetic foot wounds and hyperbaric therapy for diabetic neuropathy.
For HBOT facility access in India, see our guides to HBOT in Delhi and HBOT in Bangalore. For a national access guide, see our HBOT near me India guide.
Frequently Asked Questions
Can I do fewer than 30 sessions if I feel better?
Feeling better is a sign that Phase 1 and Phase 2 are working — not that the protocol is complete. The symptom improvement that most patients notice by session 15 to 20 reflects antibiotic potentiation and initial inflammatory reduction. The angiogenesis that prevents recurrence — the Phase 3 benefit — has not yet fully established at session 20. Stopping at session 20 produces a partial result: the infection responds but the hypovascular environment that made it refractory remains, and recurrence is common. Complete the course.
What if I miss sessions during the protocol?
Occasional missed sessions — one or two per course — do not significantly affect outcomes. The cumulative angiogenic effect builds across the course, and a single gap does not reset the progress. Consistent gaps — missing sessions twice weekly through the course — reduce the hyperoxic-hypoxic cycling frequency below the threshold needed for optimal angiogenesis. Protocol adherence should be prioritised, and missed sessions should be made up where possible.
Can sessions be done twice daily to shorten the course?
Twice-daily sessions are used in the acute phase of gas gangrene and DCS — where immediate bactericidal effect is the priority. For osteomyelitis, once-daily sessions are standard because the angiogenesis mechanism depends on the hyperoxic-hypoxic cycle — the relative hypoxia between sessions is part of the angiogenic signal. Compressing the inter-session interval with twice-daily sessions is not standard practice for osteomyelitis and does not shorten the effective course length.
How do I know if the sessions are working?
The mid-course review at session 20 to 25 provides the formal clinical assessment. Between sessions, patients can monitor symptom trajectory — reducing pain, improving mobility, decreasing discharge from associated wounds — as proxy indicators of response. Normalising inflammatory markers (CRP returning toward normal range) is a more reliable objective indicator than symptoms alone. Imaging changes are typically visible only at the mid-course or post-treatment review, not session by session.
What about sessions after the osteomyelitis course — for maintenance?
Maintenance HBOT beyond the standard course is not standard practice for osteomyelitis. The angiogenesis established during the 30 to 40 session course is self-sustaining once new vessels have matured. Patients with recurrent osteomyelitis after a completed HBOT course should be reassessed for adequacy of surgical debridement, antibiotic selection, and completeness of the original protocol — not automatically retreated with a second HBOT course.
The Session Count Is the Protocol. The Protocol Is the Therapy.
How many hyperbaric oxygen therapy sessions does osteomyelitis need? Thirty to forty — because bone angiogenesis requires that many cycles of hyperoxic-hypoxic stimulus to establish new vascularity in tissue that chronic infection has made permanently hypovascular.
The number is not conservative caution. It is the time biology requires to do what the therapy initiates. Phase 1 makes antibiotics work. Phase 2 builds the vessels that will sustain the environment. Phase 3 matures them. Stopping before Phase 3 completes means losing the prevention that makes the Phase 1 and 2 investment worthwhile.
For Indian patients managing chronic bone infection — know the full protocol before starting. Plan the 6 to 8 weeks. Commit to the complete course. And understand that the best result typically appears not at session 40, but 4 to 8 weeks after it.
The 30 to 40 session protocol for osteomyelitis is not long because osteomyelitis is hard to treat. It is long because permanent recovery requires more than symptom control — it requires rebuilding the infrastructure that allows bone to resist infection on its own. Angiogenesis takes the time it takes. The protocol is designed around biology, not convenience.
For the complete osteomyelitis protocol and evidence base, see our primary guide on HBOT for refractory osteomyelitis. For all 14 HBOT indication uses, see our HBOT uses guide.
The sessions are not the treatment. The biology they trigger is the treatment. Complete the course.




