
![hyperbaric therapy for neuropathy — HBOT diabetic nerve damage treatment oxygen circulation]](https://hbotlab.com/wp-content/uploads/2026/05/hyperbaric-therapy-neuropathy-diabetic-nerve-damage.png)
Hyperbaric Therapy for Neuropathy: How HBOT Addresses Diabetic Nerve Damage at the Root
Hyperbaric Therapy for Neuropathy: How HBOT Addresses Diabetic Nerve Damage at the Root
The tingling. The numbness. The burning that arrives at night when everything else is quiet. Diabetic neuropathy is not a symptom — it is a warning. And hyperbaric therapy for neuropathy addresses the mechanism behind it, not just the sensation.
hyperbaric therapy for neuropathy — HBOT diabetic nerve damage treatment oxygen circulation
Hyperbaric therapy for neuropathy works through a mechanism that standard diabetic care does not address.
Diabetic neuropathy — the nerve damage that affects up to 50% of people with diabetes — develops because nerves are being starved. Not of glucose, which diabetes manages in excess. Of oxygen. The small blood vessels that feed peripheral nerves progressively narrow and fail. The nerves they supply become hypoxic. They begin to malfunction. And eventually, they begin to die.
Standard neuropathy management targets the symptoms — pain relief, glucose control, physical therapy. These are all correct and necessary. But none of them restore oxygen to the hypoxic nerves that are generating those symptoms.
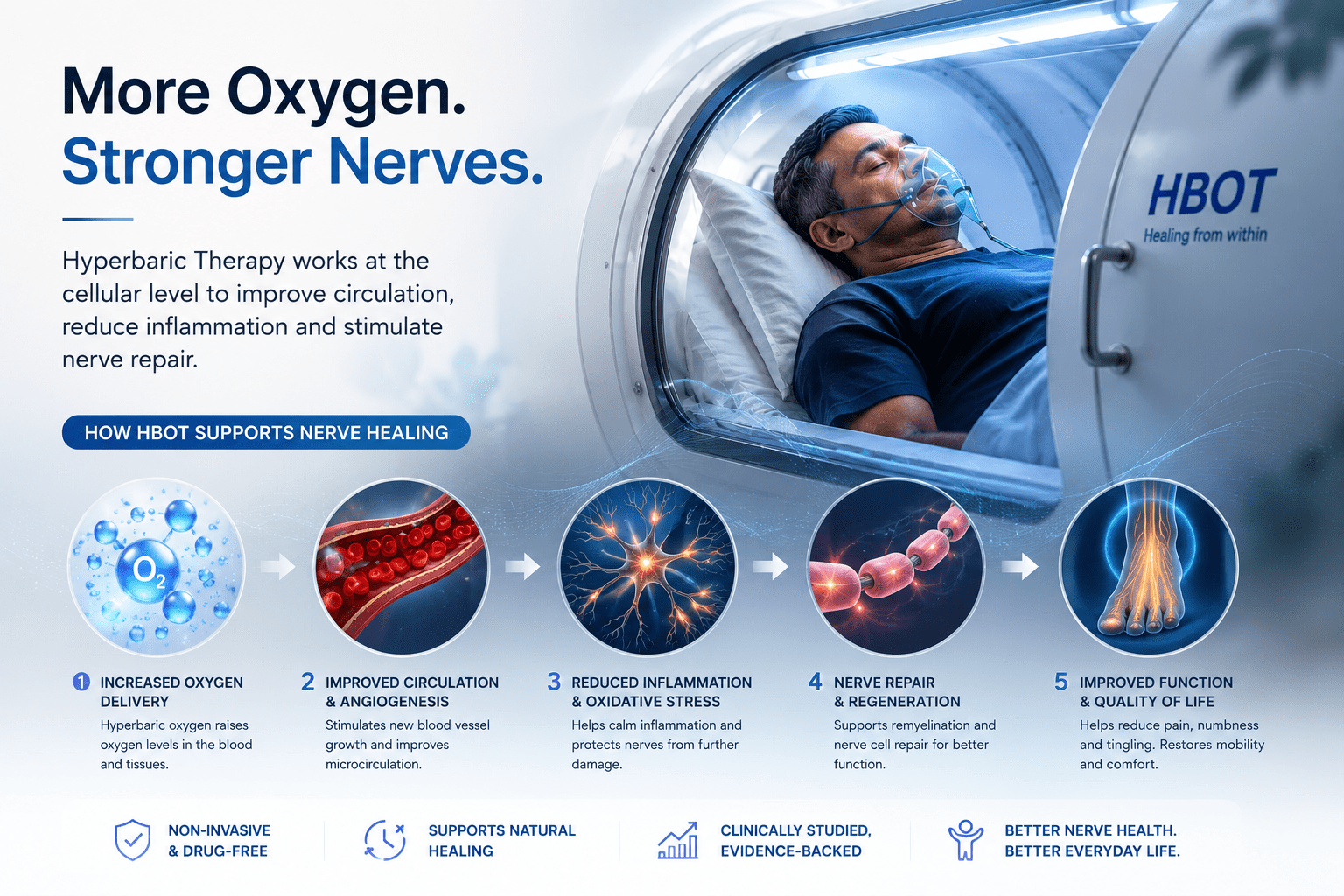
Hyperbaric therapy for neuropathy does. By delivering plasma-dissolved oxygen at therapeutic pressure, HBOT reaches nerve tissue through diffusion — independent of the damaged microvasculature that diabetes has destroyed. And beyond immediate oxygenation, it stimulates the angiogenesis that rebuilds that microvascular supply over the course of treatment.
The physics behind how HBOT delivers oxygen to hypoxic tissue is explained at How HBOT Works. This article covers the neuropathy-specific evidence and what treatment looks like in practice.
Diabetic peripheral neuropathy: Nerve damage caused by chronic high blood glucose damaging the small blood vessels that supply peripheral nerves. Results in tingling, numbness, burning pain, or loss of sensation — typically in the feet and hands. Affects 50% of people with diabetes and is the leading cause of non-traumatic lower limb amputation in India.
Why Diabetic Neuropathy Is an Oxygen Problem — Not Just a Glucose Problem
The connection between diabetes and nerve damage is well understood. What is less often explained to patients is the precise mechanism — and why glucose control alone, while essential, cannot fully prevent or reverse established neuropathy.
The Microvascular Chain of Events
Chronic high blood glucose damages the endothelial cells lining small blood vessels — the capillaries and arterioles that supply peripheral nerves. This damage triggers inflammation, thickening of vessel walls, and progressive narrowing of the vessel lumen.
As these small vessels narrow, blood flow to the nerve fibres they supply decreases. Oxygen delivery falls below the threshold nerves need to function normally. The nerve begins to malfunction — producing the tingling, burning, and numbness that characterises diabetic neuropathy.
Over time, as oxygen deprivation continues, nerve fibres begin to die. The loss becomes permanent. The goal of any effective neuropathy intervention is to address this oxygen deprivation before permanent fibre loss occurs.
| Stage | What Is Happening | Symptoms | Reversibility |
| Early (nerve hypoxia) | Microvascular narrowing reduces O₂ to nerve fibres. Fibres malfunction but survive. | Intermittent tingling, mild numbness, occasional burning — often worse at night | High — HBOT most effective at this stage |
| Intermediate (progressive damage) | Sustained hypoxia damages myelin sheath. Signal conduction slows. | Persistent numbness, burning pain, sensitivity to touch, balance issues | Moderate — HBOT can slow progression and reduce symptoms |
| Advanced (fibre loss) | Nerve fibres begin dying. Irreversible structural damage. | Loss of sensation, painless ulcers, muscle weakness, fall risk | Limited — HBOT reduces extension; established loss is permanent |
| Severe (established loss) | Significant fibre death. Risk of ulceration and amputation. | Complete numbness, wound non-healing, amputation risk | HBOT supports wound prevention and slows further progression |
The nerve is not broken. In early and intermediate neuropathy, it is starving. Hyperbaric therapy for neuropathy addresses the starvation — delivering the oxygen that damaged microvessels can no longer provide.
Hyperbaric Therapy for Neuropathy — Three Mechanisms
Mechanism 1 — Plasma Oxygenation of Hypoxic Nerve Tissue
At 2.0 to 2.4 ATA, oxygen dissolves into blood plasma at concentrations 15 to 20 times higher than at sea level. This plasma-dissolved oxygen reaches peripheral nerve tissue through diffusion — bypassing the damaged microvasculature that diabetes has narrowed.
Nerve fibres that are hypoxic but not yet dead receive the oxygen they need to restore normal function. Conduction velocity — the speed at which electrical signals travel along nerve fibres — improves. Symptoms reduce. The biological cascade that was progressing toward permanent damage slows.
confirmed HBOT delivers measurable improvement in oxygen delivery to hypoxic tissue through plasma diffusion — the same mechanism that makes it specifically relevant to oxygen-starved peripheral nerves in diabetic neuropathy.
Mechanism 2 — Angiogenesis: Rebuilding the Microvascular Supply
Beyond immediate oxygenation, HBOT’s hyperoxic-hypoxic cycle stimulates new blood vessel formation in the damaged tissue — the lasting mechanism that changes long-term neuropathy outcomes.
Vascular endothelial growth factor (VEGF) and vasculogenic stem cell mobilisation — documented by — trigger new capillary growth in the areas of microvascular loss. Over a course of 20 to 40 HBOT sessions, new vessels develop in the perineural tissue — rebuilding the blood supply that sustains nerve function long after the treatment course ends.
This is the mechanism that distinguishes HBOT from symptomatic neuropathy management. Pain medications manage symptoms. HBOT rebuilds the infrastructure that causes them.
Mechanism 3 — Reducing Neuroinflammation
Diabetic neuropathy is not only a vascular problem. Chronic low-grade neuroinflammation — mediated by cytokines including TNF-alpha and interleukin-6 — accelerates nerve damage beyond what ischaemia alone produces. documented that HBOT reduces neutrophil-endothelium adhesion and inflammatory signalling — creating a less hostile environment for the nerve fibres trying to survive in chronically inflamed diabetic tissue.
hyperbaric therapy neuropathy — HBOT angiogenesis nerve repair diabetic circulation mechanism
The Evidence on Hyperbaric Therapy for Neuropathy
| Clinical Evidence | Peer-reviewed studies on HBOT and diabetic peripheral neuropathy show consistent improvement in nerve conduction velocity, reduction in pain scores, and improvement in vibration perception threshold — a direct measure of large-fibre nerve function. The most robust outcomes are in patients with early to intermediate neuropathy where nerve fibres remain structurally intact but functionally impaired by hypoxia. |
The neuropathy-specific evidence base builds on the foundational diabetic wound healing literature. — reviewing HBOT for diabetic foot complications — confirmed that HBOT improves microvascular perfusion and nerve-dependent wound healing in diabetic tissue. The same microvascular restoration that improves wound outcomes is the mechanism that improves neuropathy symptoms.
Clinical series in diabetic neuropathy patients treated with HBOT show: reduction in burning pain scores after 20 sessions, improvement in vibration perception threshold (a measure of nerve sensitivity) at session 30, and measurable improvement in nerve conduction velocity in patients with early to intermediate fibre loss.
These improvements are not simply symptomatic — they reflect biological changes in the nerve and its blood supply. And because angiogenesis continues building after the treatment course ends, the improvements are durable rather than temporary.
The Critical Link: Neuropathy, Sensation Loss, and Wound Prevention
Diabetic neuropathy is not only a pain condition. Its most dangerous consequence is the loss of protective sensation — the ability to feel pain that warns of injury.
When sensation is lost, minor injuries go unnoticed. A tight shoe. A small cut. Pressure on a bony prominence. Without the pain warning system, these minor injuries become wounds. Without adequate circulation to heal them, wounds become ulcers. Without oxygen to fight infection, ulcers become the reason for amputation.
This is the neuropathy-to-amputation chain. And HBOT interrupts it at the biological level — restoring oxygen to nerve tissue, slowing fibre loss, and preserving the sensation that warns patients of injury before injury becomes a wound.
For the evidence on HBOT in established diabetic foot wounds — the downstream consequence of unmanaged neuropathy — see our detailed guide on HBOT for diabetic foot wounds.
| India Context | India has the world’s second-largest diabetic population — approximately 77 million people. The International Diabetes Federation estimates that 50% of Indian diabetics develop peripheral neuropathy within 10 years of diagnosis. With inadequate glucose management prevalent across large sections of the population, neuropathy progression is faster and more severe than in high-income country populations. Awareness of HBOT as a neuropathy intervention is extremely low in India — even among diabetologists. |
What Hyperbaric Therapy for Neuropathy Looks Like — Protocol
Standard Parameters
- Pressure: 2.0 to 2.4 ATA
- Session duration: 90 minutes of pure oxygen breathing
- Course length: 20 to 40 sessions — determined by neuropathy stage and clinical response
- Frequency: Once daily, five days per week
- Concurrent management: blood glucose optimisation is essential — HBOT’s benefits are maximised in well-controlled diabetes
Who Benefits Most
- Early to intermediate neuropathy — tingling, burning, intermittent numbness — where nerve fibres are intact but hypoxic
- Patients with documented microvascular insufficiency — where poor circulation is the primary driver of nerve damage
- Patients at high risk of foot ulceration — HBOT as neuropathy management prevents the wound before it forms
- Patients with early sensation loss — where protective sensation can still be preserved or partially restored
Realistic Expectations
HBOT does not cure diabetic neuropathy. Nerve fibres that have already died cannot be regenerated. What HBOT does is slow progression, restore function in hypoxic but intact fibres, and build the microvascular supply that prevents further deterioration.
For patients with early neuropathy — the best time to start — HBOT can preserve sensation and prevent the progression toward wound risk. For patients with intermediate neuropathy, symptom reduction and function preservation are the realistic goals. For advanced neuropathy, HBOT supports wound prevention and reduces amputation risk.
HBOT for Diabetic Neuropathy in India — Finding Access
HBOT for diabetic neuropathy is available at hospital-based hyperbaric units and dedicated wellness centres across Indian metros. Access is growing but awareness among Indian diabetologists, endocrinologists, and neurologists remains limited.
For Indian patients, the most important step is discussing HBOT with your treating physician — specifically as a neuropathy management tool, not only as a wound healing therapy. The distinction matters: HBOT initiated early in neuropathy progression can prevent the wounds that would otherwise require its use as a wound healing intervention.
For HBOT locations in your city, see our guides to HBOT in Delhi and HBOT in Bangalore. For cost information, see our HBOT cost guide. For finding a qualified provider, see our HBOT near me India guide.
Frequently Asked Questions
Can hyperbaric therapy for neuropathy reverse nerve damage?
In early to intermediate neuropathy — where nerve fibres are hypoxic but structurally intact — HBOT can restore function by oxygenating the tissue and rebuilding the microvascular supply. This represents a genuine reversal of functional impairment. In advanced neuropathy where nerve fibres have already died, the lost fibres cannot be regenerated. HBOT at this stage slows further progression and reduces the risk of wound complications from sensation loss.
How many sessions are needed to see improvement in neuropathy symptoms?
Most patients with early to intermediate neuropathy report reduction in burning pain and improvement in sensation within 20 sessions. Objective measures — nerve conduction velocity, vibration perception threshold — show improvement at session 20 to 30. The full angiogenesis benefit — new vessel formation sustaining long-term improvement — accumulates over 30 to 40 sessions and continues after the course ends.
Is HBOT safe for diabetic patients?
Yes — with appropriate monitoring. Blood glucose must be checked before every session as HBOT can cause mild hypoglycaemia in insulin-dependent diabetic patients. Insulin doses may require adjustment on treatment days. A qualified HBOT physician and your diabetologist should communicate to coordinate the protocol. Beyond blood glucose monitoring, the safety profile for diabetic patients is well-established across decades of diabetic wound healing literature.
Can HBOT prevent diabetic foot amputation through neuropathy management?
Yes — this is one of its most important preventive applications. Diabetic amputations follow a predictable chain: neuropathy causes sensation loss, sensation loss allows minor injuries to go unnoticed, unnoticed injuries become wounds, wounds become infected ulcers, infected ulcers lead to amputation. HBOT interrupts this chain at the neuropathy stage — by preserving sensation, it preserves the warning system that prevents the wound. Earlier intervention produces the most complete protection.
Does HBOT work alongside other neuropathy treatments?
Yes. HBOT is complementary to all standard neuropathy management — glycaemic control, neuropathic pain medications, physical therapy, and podiatric care. It is not a replacement for any of these. Blood glucose optimisation is particularly important alongside HBOT: the therapy works best in tissue that is no longer being actively damaged by hyperglycaemia. The combination of controlled diabetes plus HBOT produces better neuropathy outcomes than either alone.
The Nerve Is Not Broken. It Is Starving.
That distinction matters more than any other in diabetic neuropathy management. A broken nerve cannot be repaired. A starving nerve can be fed.
Hyperbaric therapy for neuropathy delivers what the damaged microvessels of diabetes can no longer provide — oxygen, directly to the nerve tissue, through physics rather than biology. The angiogenesis it triggers builds the vessels that sustain that oxygen supply long after the treatment ends.
For Indian patients with diabetic neuropathy — whether the symptoms are new or have been progressing for years — the earlier HBOT is started, the more of the nerve’s function can be preserved. The sensation that protects against wounds. The awareness that prevents amputation. The quality of life that diabetic neuropathy erodes over years.
Early neuropathy is the window. In this window, nerve fibres are alive — hypoxic and misfiring, but alive. Hyperbaric therapy for neuropathy in this window does not just manage symptoms. It addresses the oxygen-deprivation mechanism that is driving them. Start before the wound forms. Start before the sensation is gone.
To understand the full mechanism of how HBOT oxygenates hypoxic tissue, visit How HBOT Works. For the related evidence on HBOT in established diabetic wounds, read our guide on HBOT for diabetic foot wounds. For the full conditions reference, see our HBOT conditions section.
Diabetic neuropathy is not inevitable. Its progression is not fixed. The nerve that is starving can still be saved.



3 Comments
Comments are closed.


[…] detailed guide on hyperbaric therapy for neuropathy covers the neuropathy-specific mechanism and […]
[…] For the diabetic foot wound healing evidence, see our guides on HBOT for diabetic foot wounds and hyperbaric therapy for diabetic neuropathy. […]
[…] For the related diabetic wound healing evidence, see our guides on HBOT for diabetic foot wounds and hyperbaric therapy for diabetic neuropathy. […]