
HBOT and Brain Injury From Infection: How Hyperbaric Oxygen Therapy Supports Brain Abscess Recovery
In a controlled cohort study of 40 patients, the brain abscess reoperation rate with HBOT was 10% — compared to 45% without it. The brain that survived the infection has more capacity for recovery than it is currently showing.
hyperbaric oxygen therapy traumatic brain injury — HBOT brain abscess recovery neurological treatment
Hyperbaric oxygen therapy and traumatic brain injury from infection share one critical mechanism: both involve brain tissue that is hypoxic, inflamed, and fighting to survive.
A brain abscess is not just an infection. It is a focal destruction of brain tissue — a cavity of pus that displaces neurons, compresses surrounding tissue, raises intracranial pressure, and deprives the perinfection brain of the oxygen it needs to mount an immune response. The bacteria survive not because they are resistant to antibiotics but because the environment around them prevents antibiotics from working at therapeutic levels.
Surgery drains the abscess. Antibiotics target the organisms. Both are essential. But a third mechanism — restoring oxygen to the hypoxic brain tissue that surrounds the cavity — is what changes whether the infection resolves in one surgical episode or returns to the operating theatre.
That is what HBOT does. And the evidence on reoperation rates makes the argument more concisely than any mechanism explanation could.
For the foundational science of how HBOT delivers oxygen to hypoxic tissue, start at How HBOT Works.
Brain abscess (intracranial abscess): A focal collection of pus within the brain parenchyma — caused by bacterial, fungal, or parasitic infection. It creates a hypoxic, hypovascular environment that impairs both immune function and antibiotic efficacy. Standard treatment: surgical drainage plus prolonged antibiotic therapy. HBOT is an evidence-supported adjunct that addresses the oxygen-deprivation mechanism neither surgery nor antibiotics alone can correct.
Why Brain Abscess Resists Treatment — The Hypoxic Brain Injury Problem
Brain abscess creates an environment that actively resists the treatments directed at it. Understanding this mechanism explains why HBOT changes outcomes — and why it is not simply an add-on to standard care.
The Blood-Brain Barrier and Antibiotic Penetration
The blood-brain barrier is one of the most selective membranes in the human body. It protects the brain from toxins and pathogens — but it also restricts the passage of many antibiotics, delivering subtherapeutic concentrations to the very tissue most in need of them.
Many antibiotics have limited blood-brain barrier penetration even in healthy tissue. In a brain abscess, the tissue surrounding the cavity is also hypoxic — and antibiotic killing efficacy is oxygen-dependent. The result: antibiotics arrive at the abscess in concentrations that are already below optimal, and in a tissue environment that further impairs their bactericidal mechanism.
How Hypoxia Disables the Immune Response
Leukocyte killing — the immune system’s primary weapon against bacterial infection — depends on an oxidative burst that requires tissue oxygen tension above 30 mmHg. The perinfection brain tissue in an abscess typically has oxygen tension well below this threshold.
This means the immune cells that reach the abscess cannot mount their full bactericidal response. They are present. They are functional in terms of cell biology. But the environment has disabled their most important weapon. The infection persists not because the immune system is absent but because it cannot work.
Why Reoperation Occurs
When brain abscess recurs after initial drainage and antibiotic therapy, the cause is almost always the same: the hypoxic, hypovascular environment around the abscess cavity was never addressed. The surgery removed the pus. The antibiotics reduced the bacterial load. But the conditions that allowed the infection to establish and resist treatment remained unchanged.
The next antibiotic course faces the same impaired efficacy. The next surgical episode finds the same compromised tissue. Without restoring oxygen to the perinfection brain, the cycle continues.
| Treatment | What It Addresses | What It Cannot Address |
| Surgical drainage | Removes the abscess cavity and reduces mass effect | Does not restore oxygen to perinfection brain tissue |
| Antibiotics | Reduces bacterial load where drug concentrations are therapeutic | Impaired by hypoxia — bactericidal mechanism requires O₂ >30 mmHg |
| HBOT | Restores tissue oxygen tension; potentiates antibiotics; supports neurological recovery | Cannot replace surgery or antibiotics — must work alongside both |
A brain abscess is not primarily an antibiotic-resistant infection. It is an oxygen-deprived infection. The bacteria survive in a sanctuary that the immune system cannot fully penetrate and antibiotics cannot fully reach. HBOT restores access to that sanctuary.
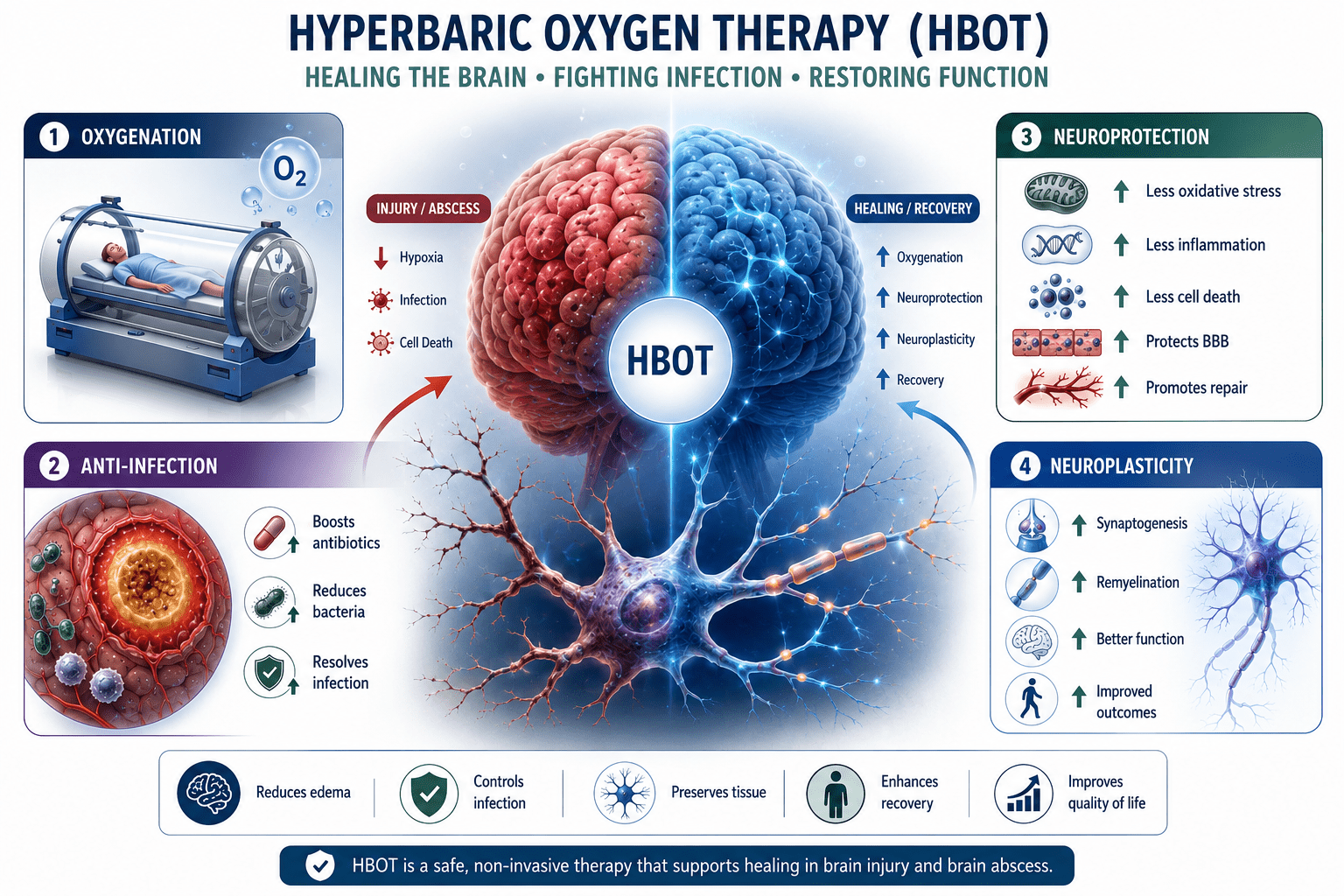
Hyperbaric Oxygen Therapy for Brain Injury: Four Mechanisms in Brain Abscess
Mechanism 1 — Restoring Tissue Oxygen to the Perinfection Brain
At 2.0 to 2.4 ATA, HBOT delivers plasma-dissolved oxygen to the hypoxic tissue surrounding the abscess cavity — restoring the oxygen tension that leukocyte killing and antibiotic efficacy require.
Tissue oxygen tension in perinfection brain rises from below 20 mmHg to above 200 mmHg during HBOT sessions — restoring the oxidative burst capacity of immune cells and enabling antibiotics to achieve their full bactericidal mechanism. established that oxygen is the limiting factor for brain recovery — confirming the mechanism that makes HBOT specifically relevant to brain tissue under ischaemic or infectious stress.
Mechanism 2 — Potentiating Antibiotic Efficacy
With tissue oxygen restored, the antibiotics being delivered systemically can now achieve therapeutic bactericidal effect in the perinfection tissue. The drug arrives. The oxygen gradient supports its mechanism. Bacterial killing proceeds at full efficacy for the first time in the treatment course.
This is not HBOT replacing antibiotics. It is HBOT making antibiotics work — addressing the oxygen-deprivation mechanism that was preventing them from working despite adequate systemic dosing.
Mechanism 3 — Neuroplasticity and Neural Dormancy Reversal
Brain infections leave neurological damage beyond the abscess cavity itself — through oedema, inflammatory mediators, and ischaemia affecting surrounding tissue. documented that hyperbaric oxygen environments enhance brain activity and neural performance — consistent with the neuroplasticity-stimulating effect of HBOT documented across multiple brain injury conditions.
Neurons in the perinfection zone are not all dead. Many are in a state of dormancy — alive but non-functional due to hypoxia and inflammation. HBOT oxygenates this dormant tissue, reducing oedema and restoring the metabolic conditions for neural reactivation.
Mechanism 4 — Stimulating New Blood Vessel Growth
Infection and inflammation destroy the microvasculature in and around the abscess cavity. Even after the infection resolves, this compromised blood supply limits long-term neurological recovery. confirmed that HBOT induces angiogenesis and nerve fibre regeneration in traumatic brain injury patients — a mechanism equally applicable to post-infectious brain injury where vascular damage limits recovery.
hyperbaric oxygen therapy brain injury — HBOT brain abscess mechanism neuroplasticity antibiotic potentiation
The Clinical Evidence — Reoperation Rates and Neurological Outcomes
| Bartek et al. 2016 | Controlled cohort study — 40 patients with brain abscess. HBOT group: reoperation rate 10%. Non-HBOT group: reoperation rate 45%. All patients in both groups achieved infection resolution. The difference was in the trajectory — patients receiving HBOT reached resolution with significantly fewer surgical interventions. The addition of HBOT to standard care produced a four-fold reduction in reoperation rate. |
The Bartek et al. (2016) data is the landmark controlled evidence for HBOT in brain abscess. The 10% vs 45% reoperation rate is not a marginal finding — it represents a fundamental difference in how the infection resolved.
The mechanism behind the difference is exactly what the biology predicts. HBOT restored tissue oxygen in the perinfection brain. Antibiotics achieved their full bactericidal effect. The immune response was no longer structurally impaired by hypoxia. The infection cleared in a single surgical and treatment episode rather than requiring repeat intervention.
| UHMS Position | The Undersea and Hyperbaric Medical Society recognises intracranial abscess as an HBOT indication — specifically as an adjunct to surgery and antibiotic therapy. The clinical rationale: HBOT addresses the hypoxic brain tissue environment that limits the efficacy of standard treatment and drives recurrence. |
What Happens to Neurological Recovery
Beyond infection resolution, patients who receive HBOT as part of their brain abscess treatment show better neurological recovery trajectories — fewer persistent cognitive deficits, better functional outcomes, and improved quality of life at follow-up.
The mechanism is the neural dormancy reversal described above. documented significant improvement in neurocognitive deficits in post-traumatic brain injury patients treated with HBOT — demonstrating the neuroplasticity mechanism that applies equally to post-infectious neurological injury.
The brain does not heal the way skin heals. Its recovery depends on neural reactivation, new vascular supply, and the restoration of metabolic conditions for function. HBOT addresses all three.
The HBOT Protocol for Brain Abscess — What Treatment Looks Like
Standard Parameters
- Pressure: 2.0 to 2.4 ATA
- Session duration: 90 minutes of pure oxygen breathing
- Course length: 20 to 40 sessions — determined by clinical and radiological response
- Frequency: Once to twice daily in the acute post-surgical phase; once daily as recovery progresses
- Concurrent with: ongoing antibiotic therapy — HBOT potentiates antibiotics, it does not replace them
- Timing: initiated as soon as the patient is neurologically stable following surgical drainage
Patient Monitoring During the Course
- MRI or CT at baseline, mid-course, and completion — tracking abscess resolution and perinfection oedema
- Neurological assessment at each session — tracking cognitive function, motor status, and language
- Inflammatory markers — CRP and white cell count — serial monitoring of systemic infection response
- Intracranial pressure monitoring where indicated — HBOT at therapeutic pressures does not increase ICP and may reduce it through oedema reduction
Brain Abscess and HBOT in India — Access and Awareness
Brain abscess in India presents with a distinct epidemiological profile compared to high-income countries. Otogenic brain abscess — arising from chronic ear infections — accounts for a significantly higher proportion of cases in India than in Western countries, reflecting the burden of untreated otitis media and mastoiditis. Rhinogenic, odontogenic, and post-traumatic abscesses are also significant.
The result is a large population of Indian patients — many of them children and young adults — presenting with brain abscesses that carry both immediate mortality risk and long-term neurological consequences. The reoperation rate in Indian neurosurgical centres — without HBOT — reflects the global non-HBOT data: recurrence in a significant proportion of cases.
Awareness of HBOT as an evidence-supported adjunct for brain abscess among Indian neurosurgeons and infectious disease specialists is limited. Most major Indian neurosurgical centres do not have hyperbaric facilities on-site — meaning the HBOT option is simply not offered to patients who would benefit.
For HBOT facility locations in India, see our guides to HBOT in Delhi and HBOT in Bangalore. For comprehensive facility guidance, see our HBOT near me India guide.
For the related evidence on HBOT in refractory osteomyelitis — which shares the oxygen-dependent antibiotic potentiation mechanism — read our article on HBOT for bone infections.
Frequently Asked Questions
Can HBOT replace surgery for brain abscess?
No. Surgical drainage is non-negotiable for brain abscesses above a threshold size — it reduces mass effect, provides diagnostic material for culture, and removes the bulk of the bacterial load. HBOT cannot drain an abscess. What it does is change the biological environment that determines whether the infection resolves after the first surgery or requires a second. HBOT should be initiated as an adjunct to, not instead of, surgical and antibiotic management.
Is HBOT safe for patients with intracranial pathology?
Yes — for neurologically stable patients. The primary concern with HBOT in brain pathology is oxygen toxicity and potential effects on intracranial pressure. At standard therapeutic pressures (2.0 to 2.4 ATA), ICP effects are modest and typically beneficial — HBOT’s vasoconstriction effect reduces cerebral oedema rather than increasing it. Patients with active seizure disorders require careful assessment before HBOT. A qualified HBOT physician and the treating neurosurgeon should review candidacy together.
How quickly does HBOT reduce the risk of brain abscess recurrence?
The Bartek et al. data showed the full benefit over a complete treatment course — patients who received HBOT had a 10% vs 45% reoperation rate at follow-up. The mechanism — restoring oxygen to perinfection tissue — begins with the first session but produces its full clinical benefit over 20 to 40 sessions. Early initiation, ideally within the first week of surgical drainage, produces the best results.
What neurological improvements can be expected?
Neurological improvement with HBOT in brain abscess follows the neural dormancy reversal mechanism — improvement in cognitive function, concentration, memory, and motor performance where these were affected by the perinfection injury. Recovery is gradual and cumulative across the course of sessions. Assessment 4 to 8 weeks after treatment completion gives the most accurate picture of neurological outcome. Not all deficits are reversible — those caused by direct tissue destruction rather than dormancy cannot be recovered. But those caused by hypoxia and ischaemia — a significant proportion — can respond to HBOT.
Does HBOT help with the neurological sequelae of brain abscess in children?
Yes — and this is a particularly important application for the Indian context given the high burden of otogenic brain abscess in paediatric populations. Children’s neuroplasticity is greater than adults — the capacity for neural recovery is higher, and HBOT’s neuroplasticity-stimulating effect is correspondingly more powerful. Paediatric HBOT is safe and well-tolerated when properly administered. Parents should discuss paediatric HBOT candidacy with the treating neurosurgeon and a qualified HBOT physician jointly.
The Brain That Survived Has More Capacity Than It Is Currently Showing
Brain abscess is survivable. With surgery, antibiotics, and modern neurosurgical care, mortality has fallen significantly. What remains — for many patients — is the neurological aftermath: the deficits that persist after the infection resolves, the cognitive changes that outlast the antibiotic course, the question of how much the brain can recover.
Hyperbaric oxygen therapy addresses this question at the biological level. Neural dormancy can be reversed. Vascular damage can be repaired. The perinfection brain that was hypoxic can receive the oxygen it needs for recovery. The infection that was driven to recur by the hypoxic environment can resolve in a single treatment episode.
The evidence is there. The mechanism is understood. For Indian families navigating brain abscess — ask specifically about HBOT. It is not experimental. It is recognised. And the reoperation data makes the case better than anything else.
The 10% vs 45% reoperation rate from the Bartek et al. study is the single most important number in this article. It means that 4 in 10 patients who did not receive HBOT needed to go back to the operating theatre. Among those who did receive HBOT, only 1 in 10 did. That difference has a name. It is called oxygen.
For the full evidence base on HBOT and brain injury, visit How HBOT Works. For the conditions overview including all neurological applications, see our HBOT conditions reference.
For the related evidence on HBOT in carbon monoxide-induced brain injury, read our guide on CO poisoning and HBOT brain protection.
The surgery saved the brain. HBOT gives it back.




