
Air in the Blood: The Medical Emergency That Only HBOT Can Definitively Treat
Drugs that dissolve blood clots cannot dissolve air bubbles. Only one therapy physically compresses intravascular gas — reducing bubble volume, restoring blood flow, and flooding ischaemic tissue with oxygen simultaneously.
arterial gas embolism HBOT treatment — hyperbaric oxygen therapy air bubble vascular emergency
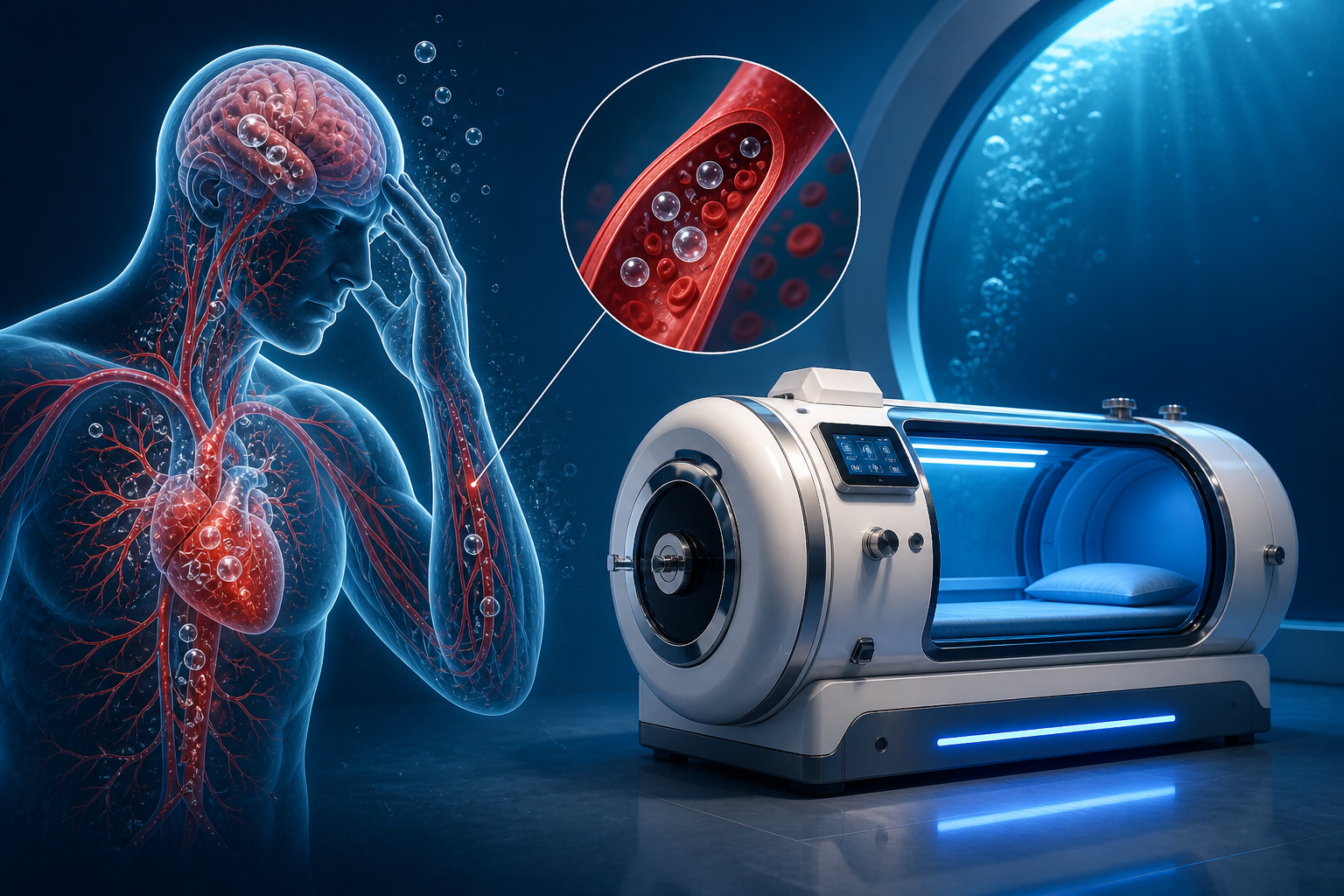
Air bubbles in the bloodstream are not a metaphor. They are literal pockets of gas blocking blood flow in arteries.
They can form during diving ascents, during cardiac or thoracic surgery, after bronchoscopy or central line placement, or wherever air gains entry to the arterial circulation. When they reach the brain, they cause stroke-like symptoms. When they reach the coronary arteries, they cause cardiac events. When they reach the spinal cord, they can cause paralysis.
The treatment is not a drug. It is not a clot-dissolving agent. Those work on fibrin — and fibrin is not what air bubbles are made of. The treatment is pressure. Physical, measurable, physics-based pressure that compresses gas bubbles according to Boyle’s Law and simultaneously floods ischaemic tissue with plasma-dissolved oxygen.
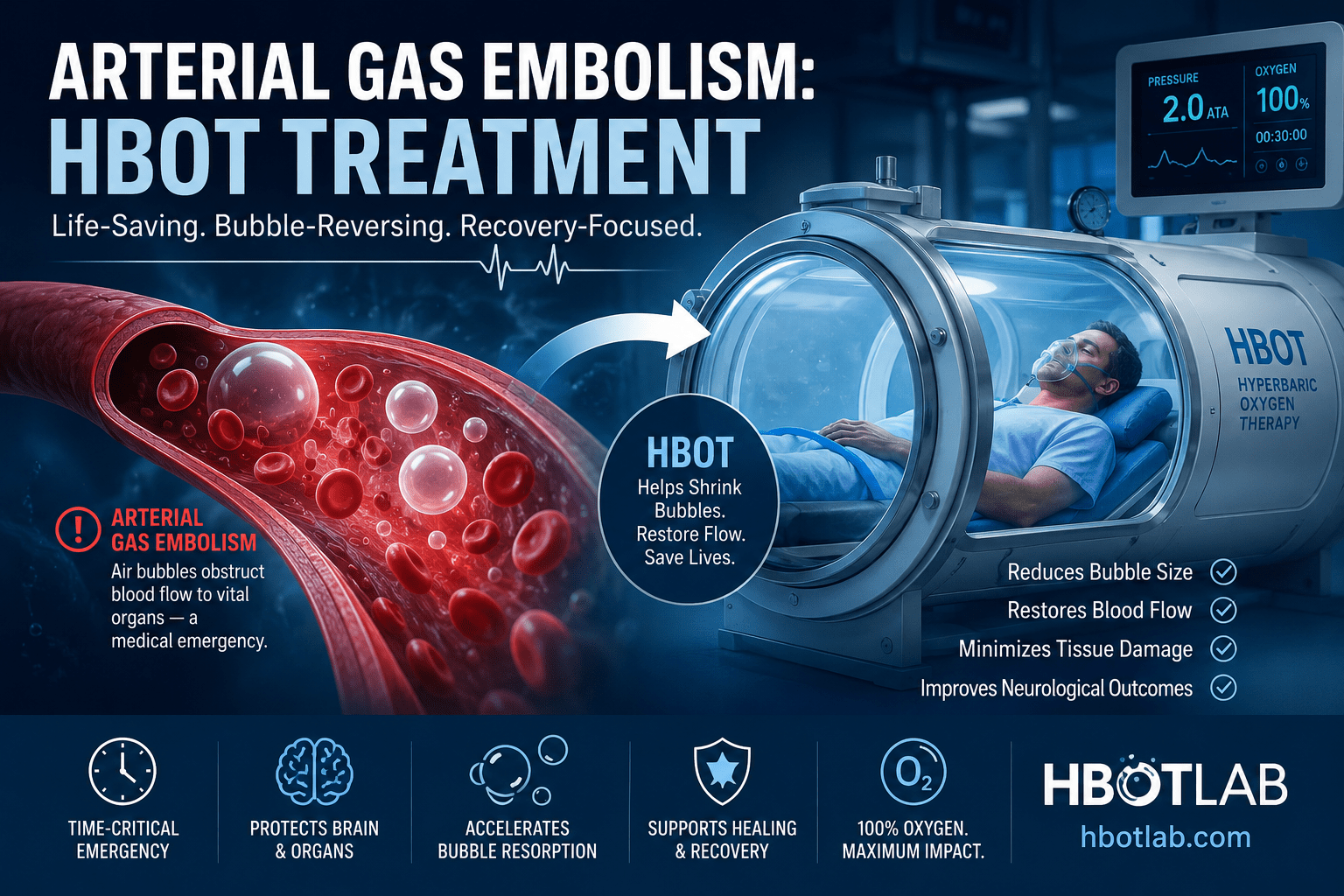
That treatment is HBOT. And in arterial gas embolism, it is not one option among several — it is the definitive treatment. The only intervention that addresses the actual physical problem.
To understand the plasma oxygenation mechanism that makes HBOT effective in vascular emergencies, read our guide on acute arterial insufficiency and HBOT.
What Arterial Gas Embolism Is — How Air Gets Into Arteries
Arterial gas embolism (AGE) occurs when gas enters the arterial circulation and travels to critical end-organs — most commonly the brain, heart, or spinal cord. The consequences depend on which arteries the bubbles reach, how large they are, and how quickly treatment is initiated.
How AGE Occurs — Sources of Intravascular Air
| Source | Mechanism | Typical Clinical Setting |
|---|---|---|
| Diving — pulmonary barotrauma | Lung overexpansion on ascent forces alveolar gas into pulmonary veins → left heart → systemic arteries | Scuba diving, breath-hold diving in some conditions |
| Cardiac surgery | Air enters coronary or cerebral arteries during cardiopulmonary bypass or valve procedures | Open heart surgery, CABG, valve replacement |
| Bronchoscopy / lung biopsy | Bronchial-venous fistula allows air entry during procedure; can cross to arterial side | Respiratory procedures, especially CT-guided biopsy |
| Central venous catheter | Air drawn into venous circulation during insertion or dressing change; large volumes can reach arterial side via patent foramen ovale | ICU, oncology, long-term venous access |
| Surgical procedures (general) | Air entry during abdominal, thoracic, or orthopaedic surgery — especially in Trendelenburg or sitting position | Neurosurgery, hip arthroplasty, laparoscopy |
| Positive pressure ventilation | Barotrauma from high airway pressures forces alveolar gas into pulmonary vasculature | ICU mechanical ventilation, especially in ARDS |
What Happens When Bubbles Reach Critical Arteries
An air bubble in a cerebral artery behaves exactly like a blood clot in that artery — it blocks flow, creates distal ischaemia, and triggers an inflammatory response at the bubble-endothelium interface. But unlike a blood clot, it does not respond to anticoagulation or thrombolysis.
The ischaemia progresses on the same timeline as any arterial occlusion — neurons begin irreversible death within minutes in affected territory. Without intervention that addresses the gas bubble directly, neurological damage accumulates.
The probability of favourable outcome in AGE decreases from 65% when HBOT is started immediately to 30% when delayed by 15 hours — a meta-analysis of 263 patients. Every hour without HBOT is an hour of accumulating neurological damage that pressure treatment can no longer reverse.
Why Drugs Cannot Treat AGE — and Why Physics Can
The Fundamental Problem With Pharmacological Treatment
The clinical instinct in any vascular emergency is to reach for drugs — anticoagulants to prevent clot extension, thrombolytics to dissolve occlusion, vasodilators to improve collateral flow. In AGE, these approaches face a fundamental limitation.
Air bubbles are not thrombotic. They are not made of fibrin. Tissue plasminogen activator dissolves blood clots by cleaving fibrin strands — it has no mechanism of action against a gas bubble. Anticoagulation prevents new clot formation around the bubble but cannot affect the bubble itself. The primary pathology — an intravascular gas bubble occupying arterial space — is untouched by pharmacology.
Only one intervention addresses a gas bubble directly: changing the pressure it exists under.
Boyle’s Law Applied Clinically
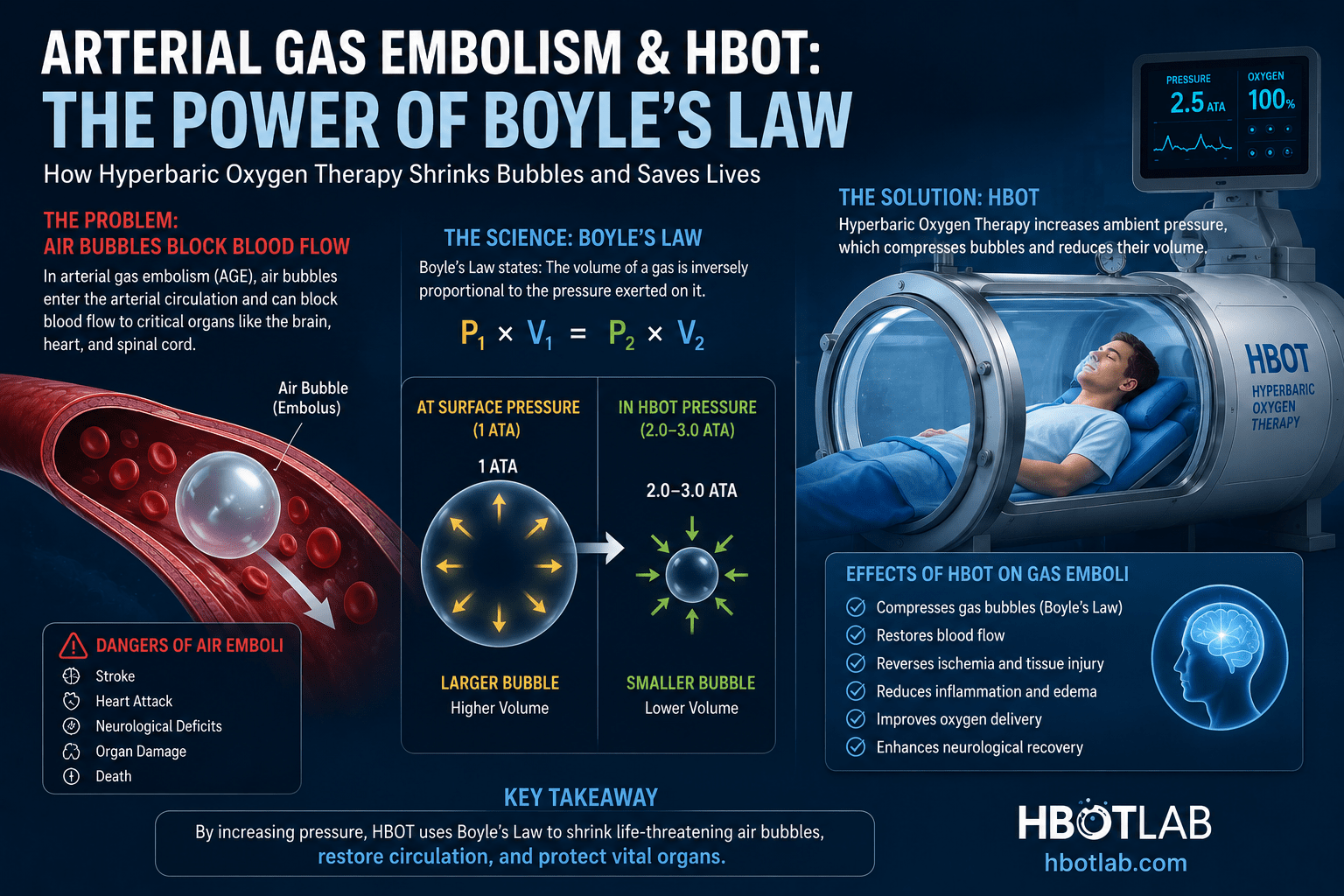
Boyle’s Law states that the volume of a gas is inversely proportional to absolute pressure at constant temperature: V₁P₁ = V₂P₂. This is not a biological concept — it is physics. It applies to gas bubbles in arteries exactly as it applies to gas bubbles anywhere else. established the foundational role of Boyle’s Law in hyperbaric medicine — pressure physically compresses intravascular gas, reducing bubble volume and restoring blood flow in occluded vessels.
| Chamber Pressure | Bubble Volume (Relative) | Blood Flow Status | Clinical Application |
|---|---|---|---|
| 1.0 ATA (surface) | 100% — full size | Occluded — full blockage | No treatment — baseline |
| 2.0 ATA (HBOT standard) | 50% of original | Partial restoration of flow | Standard HBOT pressure — first-line AGE treatment |
| 2.8 ATA (US Navy TT6) | 36% of original | Significant flow restoration | Standard decompression illness protocol — used for AGE |
| 6.0 ATA (USN TT6A) | 17% of original | Near-complete flow restoration | Severe AGE — refractory to lower pressure treatment |
A gas bubble at 1 ATA. At 2.8 ATA it is 36% of that size. At 6 ATA it is 17%. The artery it blocked is no longer blocked. Blood flows. Oxygen arrives. Physics does what pharmacology cannot.
The Combined Mechanism — Compression Plus Oxygenation
HBOT does not rely on bubble compression alone. Simultaneously with the physical reduction in bubble volume, plasma-dissolved oxygen reaches the ischaemic tissue downstream at concentrations 15 to 20 times higher than at atmospheric pressure.
The tissue that was cut off from oxygen while the bubble was full-sized — and dying with every minute — receives therapeutic oxygen through plasma diffusion while the bubble is being compressed. The two mechanisms work in parallel: one mechanical, one biological.
This dual mechanism — physical compression plus plasma oxygenation — is what distinguishes HBOT in AGE from any other available intervention. documented the anti-inflammatory actions that further reduce secondary tissue injury: neutrophil adhesion reduction, reactive oxygen species modulation, and mitochondrial protection in ischaemic cells.
 arterial gas embolism HBOT — Boyle’s Law bubble compression mechanism hyperbaric oxygen treatment
arterial gas embolism HBOT — Boyle’s Law bubble compression mechanism hyperbaric oxygen treatment
The Time Evidence — What Every Hour of Delay Costs
| Meta-Analysis — 263 AGE Patients | A 2023 PubMed meta-analysis of 263 arterial gas embolism patients documented the relationship between time to HBOT initiation and favourable outcome. Probability of favourable outcome: 65% when HBOT started immediately after AGE onset, declining to 30% when treatment was delayed by 15 hours. The evidence is unambiguous: AGE is an HBOT emergency measured in minutes, not hours. |
The timing data in AGE mirrors what is seen in decompression sickness — our article on decompression sickness and HBOT documents the same time-critical window in another diving-related gas bubble emergency. The underlying physics and biology are identical.
The clinical implication is direct: AGE is not a condition where HBOT can be arranged on the next available booking. It is a condition where every minute between diagnosis and chamber entry changes what neurological function can be preserved.
Iatrogenic AGE — The Medical Procedure Risk Most Patients Never Know About
While diving-related AGE is the most recognised form of this emergency, the majority of AGE cases in hospital settings are iatrogenic — caused by medical procedures. This is a risk that patients undergoing common interventions may not know exists, and that treating teams must be prepared to recognise and manage immediately.
The Central Venous Catheter Risk
Central venous catheters — used routinely in ICUs, oncology wards, and surgical settings for long-term venous access — carry a risk of air embolism during insertion, removal, or dressing change. When the catheter hub is open to air and the patient takes a deep breath, negative intrathoracic pressure can draw air directly into the venous circulation. In patients with a patent foramen ovale (estimated 25 to 30% of the population), venous air can cross to the arterial side — producing AGE.
Cardiac Surgery
Open-heart surgery requires discontinuation and restart of cardiac circulation — creating multiple opportunities for air entry into the coronary and cerebral arteries. Despite meticulous deairing procedures, post-cardiopulmonary bypass AGE occurs and is a recognised cause of post-operative neurological deficit.
HBOT for post-cardiac surgery AGE requires close coordination between the cardiac surgery team and the hyperbaric facility. When AGE is suspected — new neurological deficit or cardiac ischaemia after weaning from bypass — immediate HBOT referral alongside standard critical care management is the standard response.
Recognition — What AGE Looks Like After a Procedure
- Cerebral AGE: sudden confusion, stroke-like focal deficit, loss of consciousness, seizure — occurring during or within minutes of a procedure
- Coronary AGE: acute chest pain, ECG changes, haemodynamic instability — occurring perioperatively
- Spinal AGE: sudden weakness, sensory loss, or bladder dysfunction — particularly after bronchoscopy or thoracic procedures
- Skin manifestations: mottling, livedo reticularis — visible in some cases of systemic air embolism
If AGE is suspected after any medical procedure: position the patient in left lateral decubitus (Durant’s manoeuvre) to trap air in the right heart away from the pulmonary outflow tract. Administer 100% oxygen immediately. Contact the hyperbaric facility and arrange emergency transport without delay.
The HBOT Protocol for Arterial Gas Embolism
Standard Treatment Tables
- US Navy Treatment Table 6 (TT6): peak pressure 2.8 ATA — standard for most AGE presentations; total duration approximately 4 hours 45 minutes
- US Navy Treatment Table 6A (TT6A): peak pressure 6.0 ATA — reserved for severe AGE refractory to 2.8 ATA; used for rapidly progressive neurological AGE
- Repeat sessions: commonly required for AGE with significant neurological involvement — one to three sessions standard; more for persistent deficit
- Pre-hospital 100% oxygen: administered during transport via non-rebreather mask — reduces gas bubble volume by accelerating nitrogen washout from blood
What Happens During Treatment
The patient is pressurised gradually from surface pressure to the target ATA. At peak pressure, the gas bubbles have compressed to a fraction of their original volume — blood flow resumes through the previously occluded vessels. Oxygen breathed at high pressure dissolves into plasma and reaches the ischaemic tissue directly.
As pressure is maintained and then gradually reduced, the small residual gas volume is absorbed into the plasma and eliminated through normal respiratory mechanisms. The rate of decompression is controlled to prevent new bubble formation.
Most AGE patients show neurological improvement within the first session. Incomplete resolution after TT6 is an indication for immediate repeat treatment rather than waiting.
Arterial Gas Embolism in India — Awareness and Access
India’s growing diving community — primarily in the Andaman Islands, Lakshadweep, and Karnataka’s coast — represents the primary population at risk for diving-related AGE. But the larger and less-recognised risk pool is India’s rapidly expanding interventional medicine sector: cardiology, thoracic surgery, bronchoscopy, and intensive care all carry iatrogenic AGE risk.
The critical gap in India is not clinical capability — Indian cardiac surgeons and intensivists are well-trained and technically proficient. The gap is in the response pathway. When AGE occurs after a procedure in an Indian hospital, the immediate question — ‘Where is the nearest hyperbaric chamber?’ — often does not have a clear answer within the institution.
Building AGE response protocols that include immediate hyperbaric referral pathways into Indian hospitals with cardiac surgery and interventional radiology programmes is among the highest-value infrastructure changes that could improve outcomes from this time-critical emergency.
For HBOT availability in major Indian metros, see our HBOTLAB Gurgaon guide and our complete HBOT Delhi guide.
For the related physics and biology behind HBOT in gas-bubble emergencies, our article on decompression sickness and HBOT covers the same Boyle’s Law mechanism in the diving context.
Frequently Asked Questions
Is AGE the same as decompression sickness?
Related but distinct. Both involve intravascular gas bubbles and both are treated with HBOT. In decompression sickness (DCS), nitrogen comes out of solution during ascent — forming bubbles throughout the venous and arterial circulation. In arterial gas embolism, air enters the arterial circulation directly — typically through pulmonary barotrauma during diving or through a procedural route. AGE tends to produce more immediate and severe neurological effects because it directly affects cerebral and coronary arteries. Both are treated with the same HBOT protocols.
Can aspirin or blood thinners help in AGE?
Anticoagulation reduces the risk of fibrin clot formation around the gas bubble — preventing the secondary thrombotic component of AGE. It does not affect the gas bubble itself. Aspirin’s anti-platelet effect similarly reduces secondary thrombosis. Both may be used alongside HBOT but are adjunctive — they do not replace the definitive treatment of bubble compression with HBOT.
What if HBOT cannot be started immediately?
Administer 100% oxygen via non-rebreather mask immediately — this accelerates inert gas elimination from the blood, reducing bubble size and supporting tissue oxygenation during transport. Position the patient appropriately (left lateral decubitus for venous AGE). Arrange emergency transport to the nearest hyperbaric facility. Document time of onset accurately — this is critical for HBOT protocol decisions. Neurological and haemodynamic support continues throughout transport.
How many HBOT sessions does AGE require?
Most AGE cases with moderate neurological presentation resolve in one to three sessions. Severe AGE — particularly cerebral or coronary — may require five or more sessions. The treating hyperbaric physician assesses neurological status after each session and determines whether further treatment is indicated. Persistent deficit after initial treatment is an indication for continued sessions, not discontinuation.
Is AGE only a risk for divers?
No. Divers represent one population at risk — particularly from pulmonary barotrauma during ascent. The larger population at risk in a hospital context is patients undergoing cardiac surgery, bronchoscopy, central line placement, and certain laparoscopic procedures. For any patient who develops acute neurological or cardiac symptoms immediately after or during a procedure, AGE should be considered in the differential diagnosis and HBOT referral arranged urgently.
The Treatment Is Physics. The Window Is Now.
Arterial gas embolism is one of the conditions in medicine where the mechanism of the definitive treatment is the most elegantly logical of any in hyperbaric medicine. A gas bubble takes up space in an artery. Increase the pressure and the bubble gets smaller. The artery is no longer fully blocked. Blood flows. Oxygen arrives through plasma simultaneously. The ischaemic tissue that was dying begins to recover.
There is no pharmacological equivalent. There is no bypass around the physics. Boyle’s Law is not a medical hypothesis — it is a physical equation. And HBOT applies it clinically.
For patients, families, and clinicians: AGE is an emergency measured in minutes. The awareness that HBOT is the definitive treatment — and that the nearest chamber needs to be reached as fast as possible — is knowledge that directly changes outcomes.
To understand the plasma oxygenation mechanism that works in parallel with bubble compression, visit How HBOT Works.
For safety information on HBOT and who can receive it, explore our HBOT safety and risks guide.
The bubble is the problem. Pressure is the solution. Time determines what survives.



2 Comments
Comments are closed.


[…] related conditions where plasma oxygenation is critical, read our articles on arterial gas embolism and acute arterial […]
[…] physics of bubble compression at different pressures is covered in our article on arterial gas embolism HBOT treatment — which uses the same Boyle’s Law […]