
The Bends: What Happens Inside Your Body — and Why Only HBOT Can Fix It
HBOT is the primary and definitive treatment for decompression sickness. The FDA and UHMS both recognise it as standard of care — not an experimental option, not a last resort.
decompression sickness HBOT treatment — hyperbaric oxygen therapy for the bends
The joint pain starts on the ascent.
It is not the ache of exertion. It is something different — deep, building, moving from the knees to the shoulders to the elbows. Within minutes it becomes unbearable. Within the hour, it may be accompanied by numbness, weakness, or confusion.
This is decompression sickness. And if it is happening to you or someone near you, there is one thing that matters above everything else right now: every minute without treatment changes the outcome.
HBOT is not one option among several for decompression sickness. It is the treatment. The only therapy that addresses what is actually happening inside the body at the physical level. Everything else is supportive. HBOT is definitive.
Here is exactly why — and what it means for you.
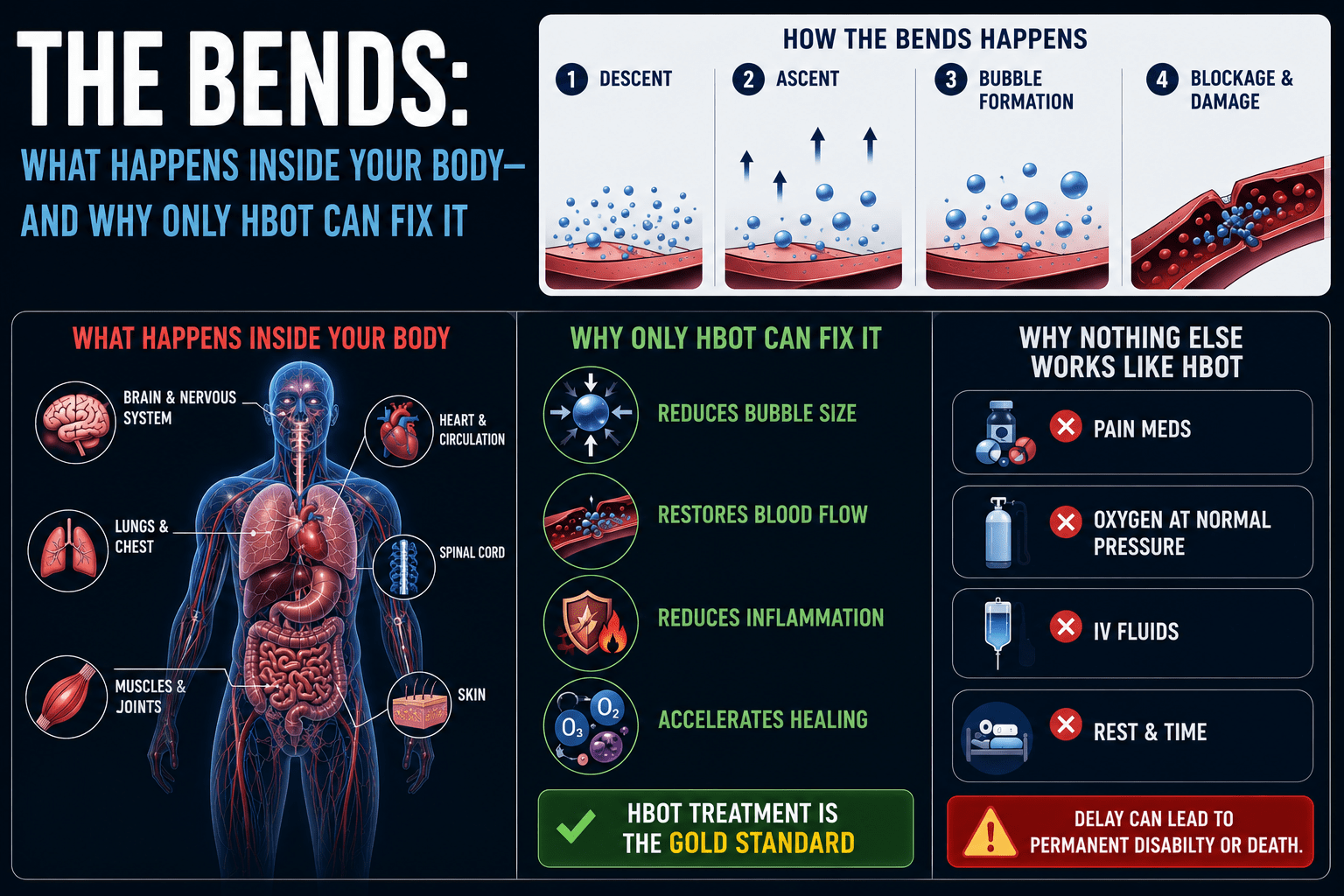
What Is Decompression Sickness — The Gas Bubble Problem
When a diver descends, the increased pressure causes nitrogen from the breathing gas to dissolve into the blood and tissues. This is normal physiology under pressure.
The danger comes on ascent. If a diver rises too quickly, the surrounding pressure drops faster than the body can eliminate the dissolved nitrogen. The gas comes out of solution — not gradually, as it should in a controlled ascent — but suddenly, forming bubbles in the blood and tissues.
These are not metaphorical bubbles. They are literal pockets of nitrogen gas forming inside your joints, your spinal cord, your inner ear, your brain. They block blood flow, damage tissue directly, and trigger an inflammatory response that compounds the injury.
| Location of Bubbles | Symptoms Produced | Risk Level |
|---|---|---|
| Joints (shoulders, knees, hips, elbows) | Deep aching pain — the classic ‘bends’ | High — most common presentation |
| Spinal cord | Weakness, paralysis, bladder dysfunction | Critical — neurological DCS |
| Brain / cerebral circulation | Confusion, visual disturbance, stroke-like symptoms | Critical — cerebral DCS |
| Inner ear / vestibular system | Vertigo, hearing loss, tinnitus | Serious — inner ear DCS |
| Lungs (pulmonary embolism pattern) | Chest pain, breathing difficulty, cough | Critical — pulmonary DCS |
| Skin | Mottling, itching, marbling pattern | Mild — Type I DCS |
The severity of decompression sickness is classified as Type I (pain only, skin) and Type II (neurological, pulmonary, vestibular). Type II presentations are medical emergencies requiring immediate treatment.
Why HBOT Is the Only Definitive Treatment
Standard oxygen therapy — a mask at normal atmospheric pressure — helps with decompression sickness in one way: it accelerates nitrogen elimination from the blood by creating a diffusion gradient. This is useful. It is not sufficient.
It does not address the physical reality of gas bubbles already present in the tissues. Oxygen at 1 ATA cannot physically compress those bubbles. It cannot reduce their volume. It cannot dissolve them back into plasma fast enough to stop the tissue damage that is continuing with every passing minute.
HBOT changes this entirely through two simultaneous mechanisms.
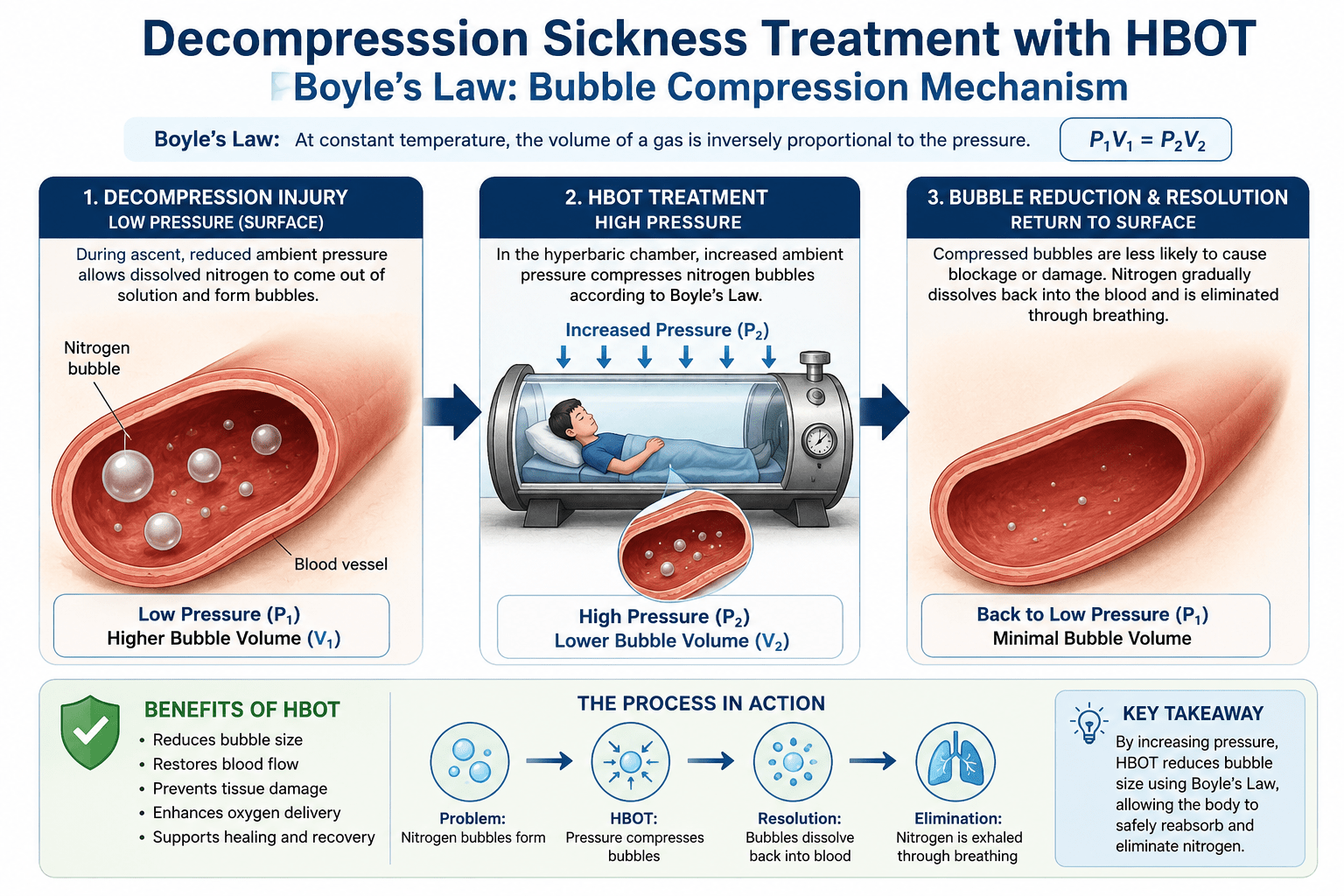
Mechanism One — Physical Compression of Gas Bubbles (Boyle’s Law)
Boyle’s Law states that the volume of a gas is inversely proportional to pressure at constant temperature. This is not a medical concept — it is fundamental physics.
At 2.0 ATA (twice normal atmospheric pressure), a nitrogen bubble occupies half its original volume. At 2.8 ATA — the pressure used in the US Navy Treatment Table 6, the global standard for DCS treatment — a bubble occupies approximately 36% of its sea-level volume.
The blood vessel that was blocked by a bubble at full size is no longer blocked. Blood flow resumes. Oxygen reaches the ischaemic tissue. The damage cascade that was progressing halts.
A nitrogen bubble at 1 ATA. At 2.8 ATA, it is 36% of that size. Physics does not change because the bubble is inside a human body. That is exactly why pressure works.
Mechanism Two — Plasma Oxygenation (Henry’s Law)
As documented by , at 2.0–2.8 ATA, oxygen dissolves directly into blood plasma at concentrations approximately 10 to 20 times higher than at normal atmospheric pressure. This plasma-dissolved oxygen reaches ischaemic tissue through diffusion — without needing functional blood flow.
While the bubbles are being physically compressed, the tissue that has been deprived of oxygen for minutes or hours is simultaneously being flooded with oxygen through plasma diffusion. Both repair processes are happening in parallel.
Mechanism Three — Reducing Bubble-Induced Inflammation
Nitrogen bubbles do not simply block blood vessels. They damage the endothelial lining of blood vessels, triggering neutrophil adhesion and an inflammatory cascade that causes secondary injury beyond the original mechanical obstruction. established that HBOT directly reduces this inflammatory response — protecting tissue at the margins of the affected area from the secondary injury that continues even after direct bubble obstruction is addressed.
decompression sickness HBOT treatment — Boyle’s Law bubble compression mechanism
The Time Window — Why Every Minute Matters in DCS
Decompression sickness is a time-critical emergency. The tissue damage caused by gas bubble obstruction accumulates with every minute of delayed treatment. Neurological DCS — where bubbles are affecting the spinal cord or brain — can cause permanent deficits if treatment is delayed by hours.
There is a clinical principle in hyperbaric medicine: treat DCS as early as possible. Even if symptoms appear to resolve spontaneously — which occasionally happens — the underlying bubble pathology may persist, and delayed presentation of more serious symptoms is documented.
The guidance is clear: do not wait to see if it improves. Seek HBOT immediately.
| UHMS Standard of Care | HBOT is the definitive treatment for decompression sickness. The Undersea and Hyperbaric Medical Society (UHMS) and the US Navy treatment protocols both specify HBOT as the primary intervention — not adjunctive, not optional. |
| FDA Recognition | Decompression sickness is one of the 14 conditions for which the US FDA has formally recognised HBOT. This is regulatory acknowledgement of an evidence base built across decades of clinical use in military, commercial, and recreational diving medicine. |
What DCS HBOT Treatment Actually Looks Like
US Navy Treatment Table 6 — The Global Standard
The Navy Treatment Table 6 (TT6) is the standard protocol for serious decompression sickness globally. It involves:
- Total duration: approximately 4 hours 45 minutes
- Peak pressure: 2.8 ATA (equivalent to 18 metres of seawater)
- Oxygen breathing periods interspersed with air breaks to reduce oxygen toxicity risk
- Option to extend the table if symptoms do not resolve — TT6 Extension adds 75 minutes
For milder Type I presentations (pain only), the shorter Navy Treatment Table 5 (TT5) may be used at the treating physician’s discretion.
Repeat sessions the following day are common for incomplete resolution. Most DCS cases require one to three sessions for full resolution; severe neurological cases may require more.
What to Do Before Reaching a Chamber
While transport to a hyperbaric chamber is being arranged:
- Administer 100% oxygen via a non-rebreather mask at the highest available flow rate — this accelerates nitrogen elimination from the blood
- Keep the patient horizontal — do not allow them to sit or stand upright if neurological symptoms are present
- Maintain hydration with oral fluids if the patient is conscious and able to swallow — dehydration worsens DCS outcomes
- Do not administer aspirin or NSAIDs without medical guidance in neurological DCS cases
- Contact the nearest DAN (Divers Alert Network) emergency line for guidance and to locate the nearest hyperbaric chamber
Recognising Decompression Sickness — Symptoms Every Diver Must Know
DCS symptoms can appear within minutes of surfacing or be delayed by several hours. Any symptom appearing within 24 hours of a dive should be treated as potentially DCS-related until proven otherwise.
Type I DCS — Pain and Skin
- Deep, aching joint pain — most commonly shoulders, elbows, knees, hips
- Skin mottling, marbling, or rash — particularly on the torso
- Localised swelling or tenderness
- Do not underestimate Type I. Pain-only DCS can progress to Type II without warning.
Type II DCS — Neurological, Pulmonary, Vestibular
- Weakness or paralysis in any limb
- Numbness, tingling, or loss of sensation
- Bladder or bowel dysfunction
- Vertigo, hearing loss, or ringing in the ears
- Chest pain, cough, shortness of breath
- Confusion, visual disturbance, difficulty speaking
- Extreme fatigue disproportionate to the dive profile
Any Type II symptom is a medical emergency. HBOT within the first few hours significantly changes the neurological outcome.
Decompression Sickness and India — What Divers Need to Know
India’s dive community is growing rapidly. The Andaman and Nicobar Islands, Lakshadweep, Netrani Island in Karnataka, and the reefs around the Gulf of Mannar are attracting increasing numbers of recreational and technical divers each year.
What has not grown at the same pace is hyperbaric infrastructure near these dive sites. The nearest fully equipped hyperbaric chamber to some of India’s most popular dive locations may be hours away by boat and air.
This is not a reason to avoid diving. It is a reason to dive with this knowledge firmly in place.
What Every Indian Diver Should Have Before Entering the Water
- The location and contact number of the nearest hyperbaric chamber
- A DAN Asia-Pacific membership — emergency hotline: +65 6630 8989
- A dive computer with proper decompression algorithms — not just a depth gauge
- A non-rebreather oxygen kit accessible on the boat
- Knowledge of the emergency transfer protocol from the dive site to the nearest chamber
For HBOT availability in Indian cities, visit our and our guide on .
Prevention — Because Not Needing HBOT Is the Best Outcome
HBOT is the definitive treatment when DCS occurs. But DCS is largely preventable with disciplined dive practice.
The Practices That Prevent DCS
- Ascend slowly — the universal standard is no faster than 9 metres per minute in the final 15 metres
- Observe safety stops — 3 minutes at 5 metres on every dive, regardless of profile
- Use dive tables or a reliable dive computer — never exceed no-decompression limits without proper decompression training and equipment
- Stay hydrated — dehydration increases DCS risk by reducing gas elimination efficiency
- Avoid flying within 18–24 hours after diving — cabin pressure changes can trigger bubble formation
- Allow adequate surface intervals between dives — repeat dives accumulate nitrogen load
- Never skip decompression stops — even if the urge to surface is strong
Frequently Asked Questions About DCS and HBOT
Can DCS resolve on its own without HBOT?
Mild Type I DCS (skin symptoms, minor joint pain) occasionally improves with rest and oxygen administration alone. However, UHMS guidelines recommend HBOT for all presentations of DCS because: symptoms that appear to resolve can recur or progress, subclinical nitrogen bubble load may persist without HBOT, and neurological tissue damage continues at the microscopic level even when gross symptoms improve. The risk of undertreating DCS is significantly greater than the risk of HBOT itself.
Is HBOT safe for DCS treatment?
Yes. HBOT for DCS is one of the most well-established applications in all of hyperbaric medicine, with a safety record built across more than six decades of military and civilian use. The most common side effects are ear pressure during pressurisation (equivalent to descending in a plane) and occasional mild claustrophobia, both of which are manageable. Oxygen toxicity at therapeutic pressures is rare and is mitigated by the air breaks built into treatment protocols.
What if HBOT is not available nearby?
Administer 100% oxygen immediately and arrange emergency transfer to the nearest chamber. Oxygen administration during transport significantly improves outcomes by accelerating nitrogen elimination and partially oxygenating ischaemic tissue. Contact DAN (Divers Alert Network) — they operate 24-hour emergency hotlines and can assist with locating chambers and coordinating transport.
Can a diver return to diving after DCS?
This requires individual medical assessment by a diving medicine physician. Return to diving after DCS depends on the severity of the episode, the completeness of recovery, the probable cause of the DCS, and the type of diving planned. Many divers return to recreational diving after full recovery from mild DCS. After serious neurological DCS, a minimum of three months and full neurological evaluation is typically required before any consideration of return.
How many HBOT sessions are needed for DCS?
Most cases of DCS resolve in one to three HBOT sessions. Severe neurological or spinal cord DCS may require five to ten sessions or more. The treating physician evaluates response after each session. The goal is resolution of all symptoms — partial improvement is not sufficient to discontinue treatment.
The Treatment Exists. The Variable Is Access.
Decompression sickness is one of the clearest examples in all of medicine of a condition with a definitive, well-evidenced treatment. The physics are unambiguous. The clinical protocols are standardised. The outcome data spans decades.
What changes outcomes for Indian divers is not the existence of HBOT — it is knowing where the nearest chamber is before getting in the water, and knowing what to do in the minutes between symptom onset and treatment.
That knowledge is now yours.
To understand how HBOT works at the biological level — including the plasma oxygenation mechanism central to DCS treatment — visit .
For HBOT cost and access information in India, see our guide.
Know your nearest chamber. Know the signs. Dive informed.



3 Comments
Comments are closed.


[…] timing data in AGE mirrors what is seen in decompression sickness — our article on decompression sickness and HBOT documents the same time-critical window in another diving-related gas bubble emergency. The […]
[…] For the full decompression sickness treatment protocol and evidence, see our guide on decompression sickness HBOT treatment. […]
[…] For the complete clinical evidence behind why HBOT works for DCS, see our guide on decompression sickness HBOT treatment. […]