
HBOT Indications: Why Necrotising Fasciitis Is the Most Time-Critical Emergency
There are 14 formally recognised HBOT indications. Some are chronic conditions treated over weeks. Some are acute emergencies treated over days. NSTI is the one where the difference between a first session at hour six and a first session at hour twelve is counted in limbs — and sometimes in lives.
hbot indications — necrotising fasciitis most urgent emergency NSTI survival six hour window
HBOT indications span the full spectrum of medical emergency — from chronic osteomyelitis treated over six weeks to decompression sickness treated over hours.
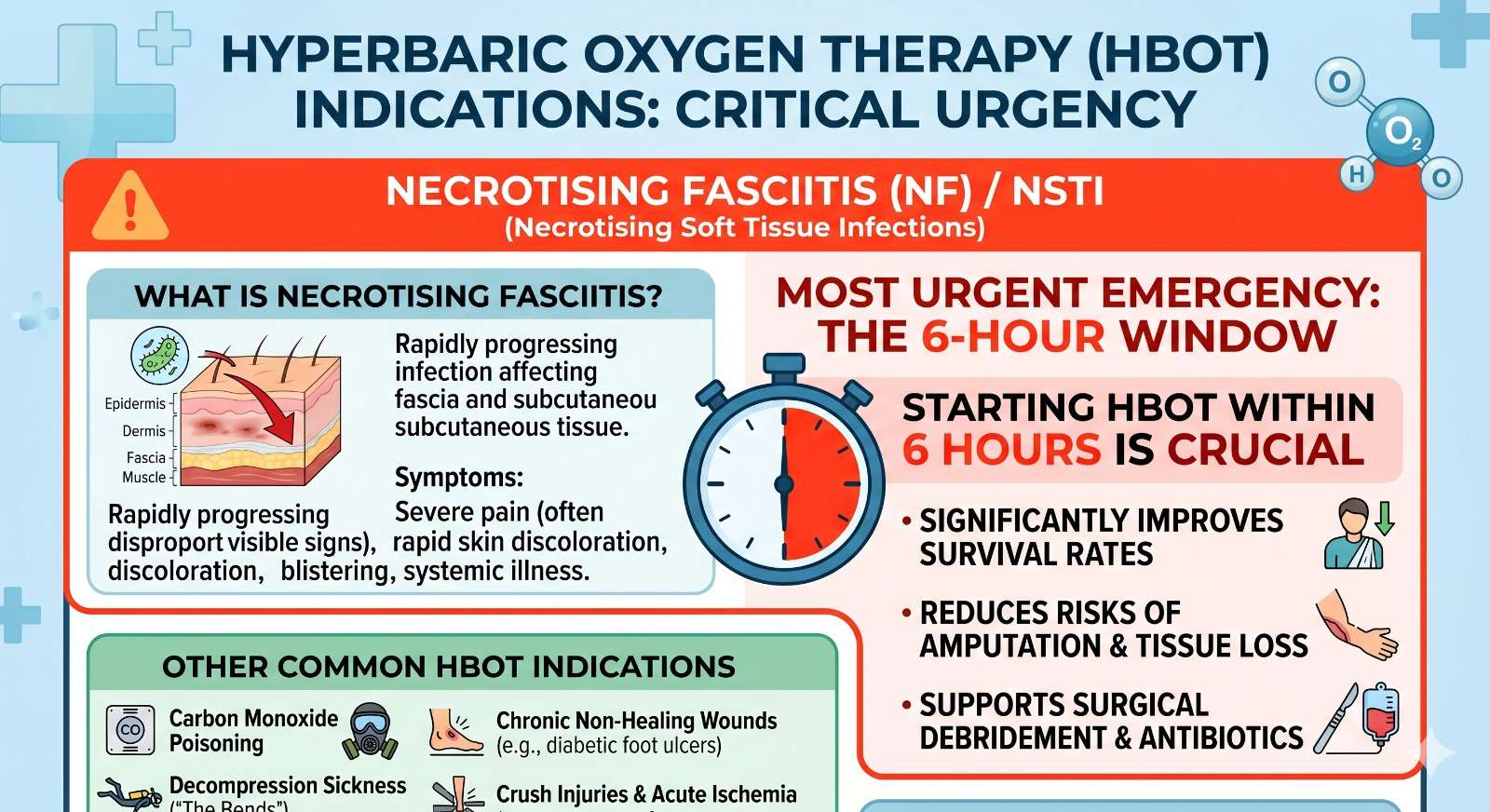
Necrotising soft tissue infection sits at the most acute end of that spectrum. Not because it is the most common HBOT indication — it is not. But because the biology of NSTI produces a time-sensitivity that no other indication matches: the bacteria spread faster, the toxins destroy more thoroughly, and the synergistic combination of aerobic and anaerobic organisms creates a multi-mechanism assault that standard treatment alone cannot contain.
Understanding NSTI in the context of all HBOT indications — what makes it different, why the six-hour window is decisive, and what the evidence shows about outcomes — is the purpose of this article. For families, surgeons, and emergency physicians managing NSTI in India, that context is not academic. It is the difference between what is possible and what gets missed.
For the primary NSTI evidence and treatment protocol, see our guide on HBOT for necrotising fasciitis survival. For the complete 14-indication overview, see our HBOT uses guide.
HBOT indications: The 14 conditions formally recognised by the US FDA and Undersea and Hyperbaric Medical Society as appropriate uses of hyperbaric oxygen therapy. Each indication reflects a specific biological mechanism where the delivery of high-concentration oxygen under pressure produces measurable clinical benefit not achievable by standard treatment alone. Necrotising soft tissue infections are among the most time-sensitive of these 14 recognised indications.
The 14 HBOT Indications — Where NSTI Sits in the Urgency Spectrum
The 14 HBOT indications fall into four urgency categories. Understanding where each falls explains why NSTI requires a different institutional response from most other indications — and why the referral decision cannot wait for surgery to be completed.
| Urgency Tier | Indications | Time Window | What Determines Outcome |
| Tier 1 Immediate — hours | Decompression sickness, Arterial gas embolism, Carbon monoxide poisoning | 1–6 hours from event | Every hour of delay worsens outcome; chamber must be available within transfer distance |
| Tier 2 Urgent — hours to 12h | Necrotising fasciitis (NSTI), Gas gangrene, Crush injury with reperfusion | 3–12 hours from injury/diagnosis | Six-hour window is the benchmark; each hour allows bacterial spread or toxin accumulation |
| Tier 3 Sub-acute — days | Acute arterial insufficiency, Arterial gas embolism residual, Severe anaemia | Within 24–72 hours | Initiation within days prevents permanent tissue loss; less strict hour-by-hour window |
| Tier 4 Chronic — weeks | Refractory osteomyelitis, Radiation injury, Diabetic wounds, Skin grafts | Within treatment course | Timing within weeks matters; angiogenesis is cumulative and session-count dependent |
NSTI occupies a unique position in the HBOT indications spectrum: it has the urgency of a Tier 1 emergency but the biological complexity of a Tier 2 infection. The bacteria spread at several centimetres per hour. The window to intercept the synergistic toxin cascade is measured not in days but in hours after the surgical decision is made.
What Makes NSTI Different From Other HBOT Indications
Each of the 14 HBOT indications has a distinct biological mechanism. NSTI’s mechanism is what makes it the most demanding indication to manage optimally — not because the therapy is harder to administer, but because the organism-specific biology creates simultaneous crises that no single treatment modality addresses completely.
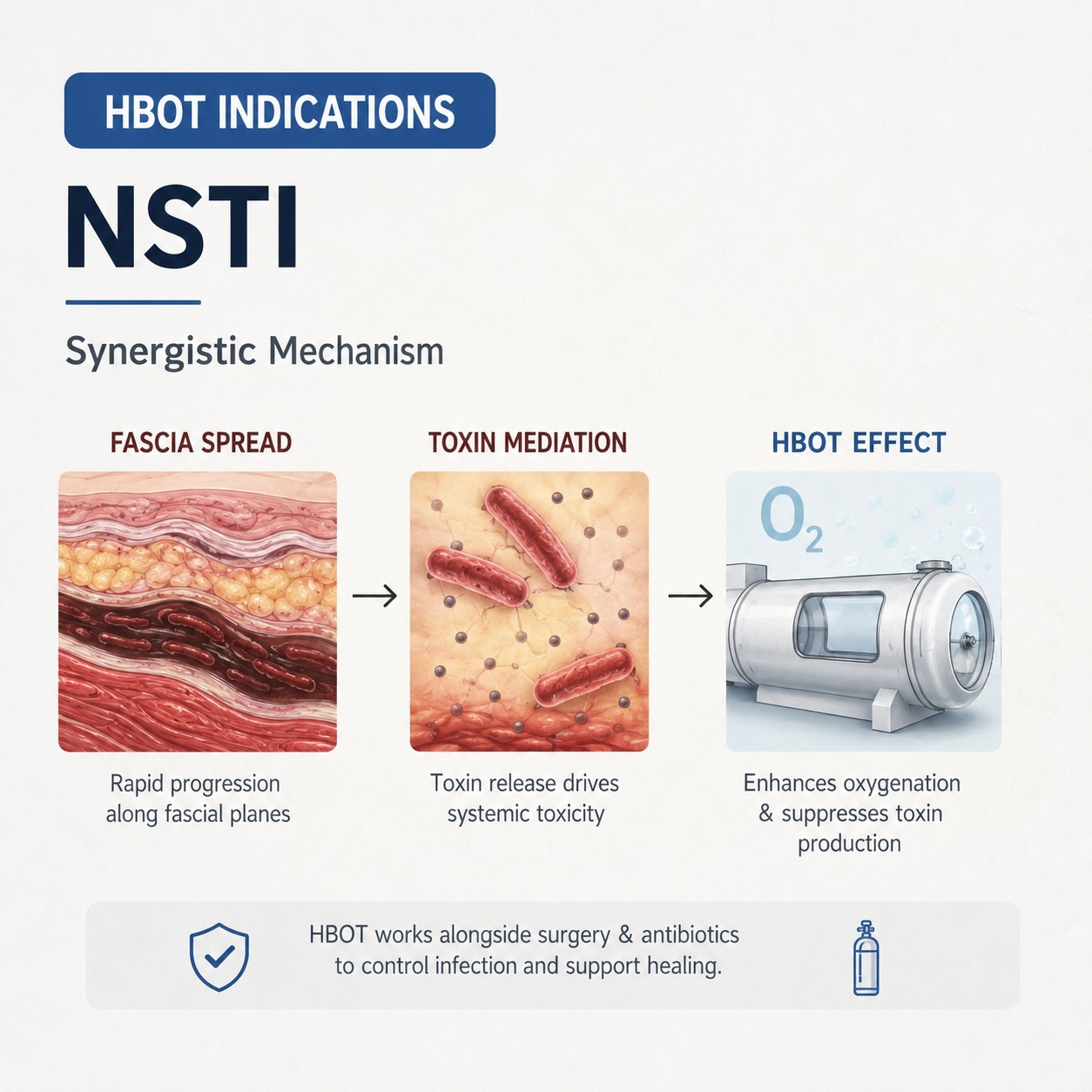
The Synergistic Pathogen Problem
Unlike gas gangrene — where the causative organism is exclusively Clostridial — NSTI typically involves a synergistic combination of aerobic and anaerobic bacteria. Group A Streptococcus, Staphylococcus aureus, Enterobacteriaceae, and obligate anaerobes act together, each creating conditions that support the other’s survival and spread.
The aerobic organisms consume local oxygen, creating the hypoxic environment that allows anaerobes to thrive. The anaerobes produce tissue-destructive enzymes that destroy blood vessels and fascia, removing barriers to aerobic spread. Standard antibiotics address individual organisms. The synergistic mechanism continues until the tissue environment is changed.
The Fascia Spread Problem
Unlike most infections — which are contained by local tissue planes — NSTI spreads along the fascial layers between tissue compartments. Fascia has minimal blood supply, which means minimal immune cell access, minimal antibiotic penetration, and minimal ability to contain the spread once established. The infection can travel tens of centimetres along a fascial plane with no external sign at the skin surface.
This is why NSTI mortality remains high even with aggressive surgical debridement: the infection is always ahead of the knife. HBOT addresses the tissue environment throughout the affected field — not just at the visible wound margins.
The Systemic Toxin Problem
NSTI pathogens — particularly Group A Streptococcus — produce pyrogenic exotoxins and other systemic toxins that cause septic shock independently of the local infection burden. Toxin production is suppressed in aerobic environments. documented the oxygen-dependent toxin suppression mechanism — applicable to both Clostridial and Streptococcal toxins. HBOT raises tissue oxygen throughout the infection field, suppressing toxin production at every site — not just where the surgeon has already debrided.
hbot indications NSTI — synergistic mechanism fascia spread toxin suppression HBOT
HBOT Indications Evidence for NSTI — The Mortality Numbers
| Mortality Benchmark | Surgery alone for NSTI: 30–50% mortality across published series. Surgery plus antibiotics plus HBOT initiated within 6 hours: multiple series documenting 10–15% mortality. For Fournier’s gangrene — the perineal variant of NSTI with the highest baseline mortality — the mortality reduction with HBOT is the most pronounced in the published literature. The six-hour window is the variable that most strongly predicts which outcome category a patient falls into. |
reviewed the evidence for HBOT across all recognised indications, confirming NSTI as a well-established indication with documented survival benefit. The anaerobic bactericidal mechanism, toxin suppression, and leukocyte potentiation that make HBOT effective for gas gangrene apply equally to the anaerobic component of NSTI — with the additional benefit that HBOT addresses the whole infection field, not just the surgically debrided area.
No randomised controlled trial exists for NSTI HBOT — the mortality without treatment makes placebo randomisation unethical. The evidence base is observational but large, spanning more than four decades and multiple countries.
The Six-Hour Window in the India Context
India’s NSTI burden is substantial — driven by high rates of diabetes, tropical climate, delayed presentation, and limited access to combined surgical and hyperbaric management. The mortality outcomes currently achieved in Indian hospitals managing NSTI reflect the structural gap between where HBOT evidence sits and where Indian emergency surgical care is delivered.
The practical constraint is not awareness of HBOT as an indication for NSTI — it is the logistical reality that most Indian tertiary surgical centres do not have on-site hyperbaric facilities, and the transfer pathway to a chamber is not established as part of the NSTI management protocol.
For Indian emergency surgeons and trauma teams managing NSTI: the referral decision should be made in the same conversation as the surgical plan — not after the operating theatre has closed. The six-hour window from initial diagnosis to first HBOT session is the benchmark that separates the outcomes observed in optimal-management series from the outcomes currently common in India.
For HBOT facility locations in India, see our guides to HBOT in Delhi and HBOT in Bangalore. For a national access guide, see our HBOT near me India guide.
NSTI vs Related HBOT Indications — Key Distinctions
NSTI shares mechanisms with gas gangrene and crush injury — which is why understanding the distinctions matters for clinical decision-making.
NSTI vs Gas Gangrene
Gas gangrene is caused exclusively by Clostridium species — obligate anaerobes. The mechanism is purely anaerobic. NSTI is synergistic — mixed aerobic and anaerobic organisms. Both benefit from HBOT’s anaerobic bactericidal mechanism, but NSTI also benefits from HBOT’s ability to inhibit the aerobic component’s creation of the hypoxic environment. Gas gangrene spreads faster in muscle. NSTI spreads faster along fascia. Both require HBOT initiation within 6 to 12 hours.
For the gas gangrene mechanism and evidence, see our guide on HBOT for gas gangrene and clostridial myonecrosis.
NSTI vs Crush Injury
Crush injury produces reperfusion injury — a different mechanism from NSTI’s synergistic infection. The time window is similar (6 hours), but the biological target is different. For crush injury, HBOT modulates the inflammatory reperfusion cascade. For NSTI, it directly kills anaerobes, suppresses toxins, and restores immune function.
For the crush injury evidence, see our guide on HBOT for crush injury and compartment syndrome.
NSTI vs Osteomyelitis
Osteomyelitis is a chronic indication — treated over 30 to 40 sessions across 6 to 8 weeks. NSTI is an acute emergency indication — treated over 10 to 20 sessions across 7 to 14 days, with the most intensive protocol in the first 24 to 48 hours. The anaerobic bactericidal mechanism is shared, but the urgency, protocol intensity, and clinical context are completely different.
For the osteomyelitis protocol detail, see our guide on HBOT for refractory osteomyelitis.
Frequently Asked Questions
Is NSTI a recognised HBOT indication in India?
Yes — NSTI is formally recognised by the UHMS and FDA as an HBOT indication, and Indian hyperbaric centres follow the same international protocols. The issue in India is not recognition of the indication but access to facilities within the time window. NSTI cases are treated at Indian hyperbaric centres, but the referral pathway is not as established as in countries with co-located surgical and hyperbaric facilities.
How many HBOT sessions are needed for NSTI?
The standard NSTI protocol is twice daily for the first 48 hours — three sessions in the first 24 hours where possible — then once daily until clinical control is achieved. Total sessions typically range from 10 to 20 over 7 to 14 days. The intensive first 48-hour protocol is what distinguishes NSTI management from most other HBOT indications and reflects the speed of bacterial spread in the acute phase.
Can HBOT be given to a patient who is still in the ICU after NSTI surgery?
Yes — critically ill patients can receive HBOT with appropriate monitoring and ventilator-compatible chamber equipment. Modern multi-place hyperbaric chambers accommodate ventilated patients, IV lines, and monitoring equipment. The clinical team coordinates session timing with ICU management. The need for ICU support is not a contraindication to HBOT — it is a reason to ensure the chamber facility is equipped for critical care patients.
What is Fournier’s gangrene and does it respond to HBOT?
Fournier’s gangrene is necrotising fasciitis of the perineum and genitalia — the NSTI variant with the highest published mortality (40 to 80% without optimal combined treatment). It responds to HBOT through the same mechanisms as other NSTI presentations, and the published mortality reduction with HBOT is most pronounced for Fournier’s gangrene across multiple series. The perineal anatomy — rich in fascial planes — creates the rapid spread pattern that makes early HBOT particularly impactful.
Is HBOT for NSTI covered by insurance in India?
Coverage for acute emergency HBOT indications varies by insurer and policy. For current guidance, see our HBOT insurance India guide.
The Indication That Cannot Wait
There are 14 HBOT indications. Most can accommodate the time it takes to arrange a referral, explain the therapy, and plan a course. NSTI cannot.
The biology does not pause while the referral is being arranged. The bacteria continue to spread along the fascia. The toxins continue to accumulate systemically. Each hour after the surgical decision that passes without HBOT initiation is an hour of synergistic infection that the therapy will have to overcome rather than prevent.
For Indian emergency and surgical teams managing NSTI: the six-hour window is the most important clinical variable you control. The decision to refer — and the activation of the transfer pathway — belongs in the same hour as the decision to operate.
The mortality reduction documented for NSTI with optimal combined treatment — surgery, antibiotics, and HBOT initiated within 6 hours — is 30–50% down to 10–15%. That gap represents lives. The mechanism is documented. The evidence is four decades deep. The question is whether the referral pathway can be activated before the window closes.
For the primary NSTI clinical evidence and protocol, see our guide on HBOT for necrotising fasciitis survival. For the complete 14-indication uses reference, see our HBOT uses guide.
Fourteen indications. One where the window is six hours. Make the call in the same hour you make the surgical decision.




