
Is HBOT Safe? A Complete Guide for Divers and Decompression Sickness Patients
It is one of the safest medical procedures in existence — with a serious adverse event rate of less than 1 in 10,000 sessions. The question is not whether HBOT is safe. It is whether the diver gets to a chamber in time.
is hbot safe — divers decompression sickness guide hyperbaric oxygen therapy risks benefits
Is HBOT safe? For divers managing decompression sickness, the honest answer matters more than the reassuring one.
The answer is yes — HBOT is safe, well-tolerated, and has a serious adverse event rate of less than one per ten thousand sessions across decades of clinical use. For divers, the more important safety question is not about the therapy. It is about delay. Decompression sickness left untreated — or treated too late — causes permanent neurological damage that no subsequent HBOT can reverse.
This article covers both: the safety profile of HBOT itself, and the safety consequences of not reaching a chamber in time after a dive.
For the full decompression sickness treatment protocol and evidence, see our guide on decompression sickness HBOT treatment.
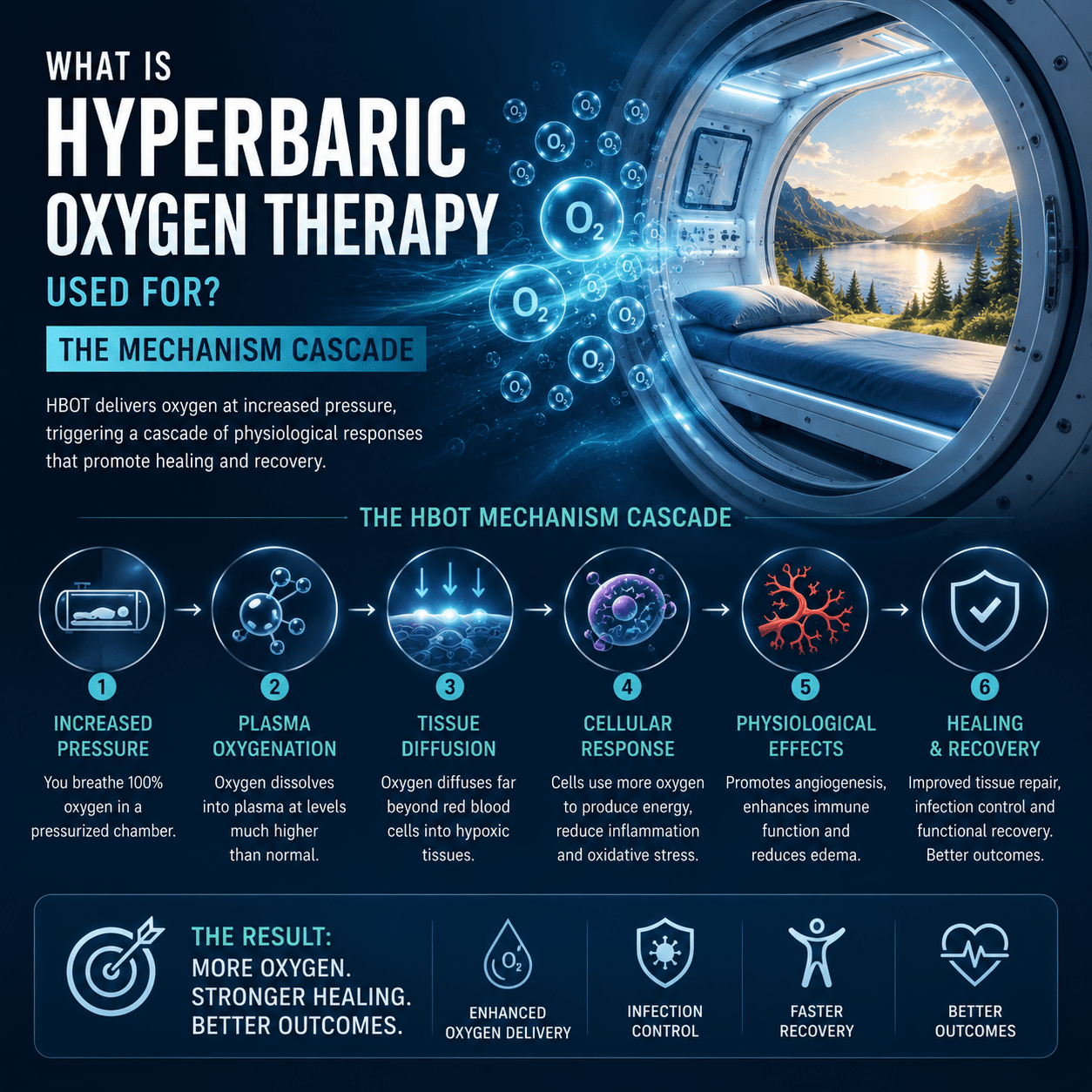
Decompression sickness (DCS): A condition caused by nitrogen bubbles forming in body tissues and blood when a diver ascends too quickly. Bubbles obstruct circulation and cause tissue damage. Symptoms range from joint pain and skin rash to paralysis and loss of consciousness. HBOT is the definitive treatment — compressing bubbles through Boyle’s Law and oxygenating the affected tissue.
Is HBOT Safe? The Evidence Across Six Decades of Clinical Use
The therapy has been used clinically since the 1960s. The accumulated safety data across millions of sessions globally makes it one of the most thoroughly characterised therapies in medicine.
Serious Adverse Events — The Real Numbers
The most comprehensive safety analyses of HBOT place the rate of serious adverse events — oxygen toxicity seizures, severe barotrauma, pulmonary complications — at less than 1 per 10,000 sessions. This is a safety profile that compares favourably with most pharmacological treatments and many surgical procedures.
The foundational safety data is summarised by — a comprehensive update on appropriate indications and safety evidence confirming HBOT as well-tolerated across its recognised indications, including decompression sickness.
Common Side Effects — Mild and Reversible
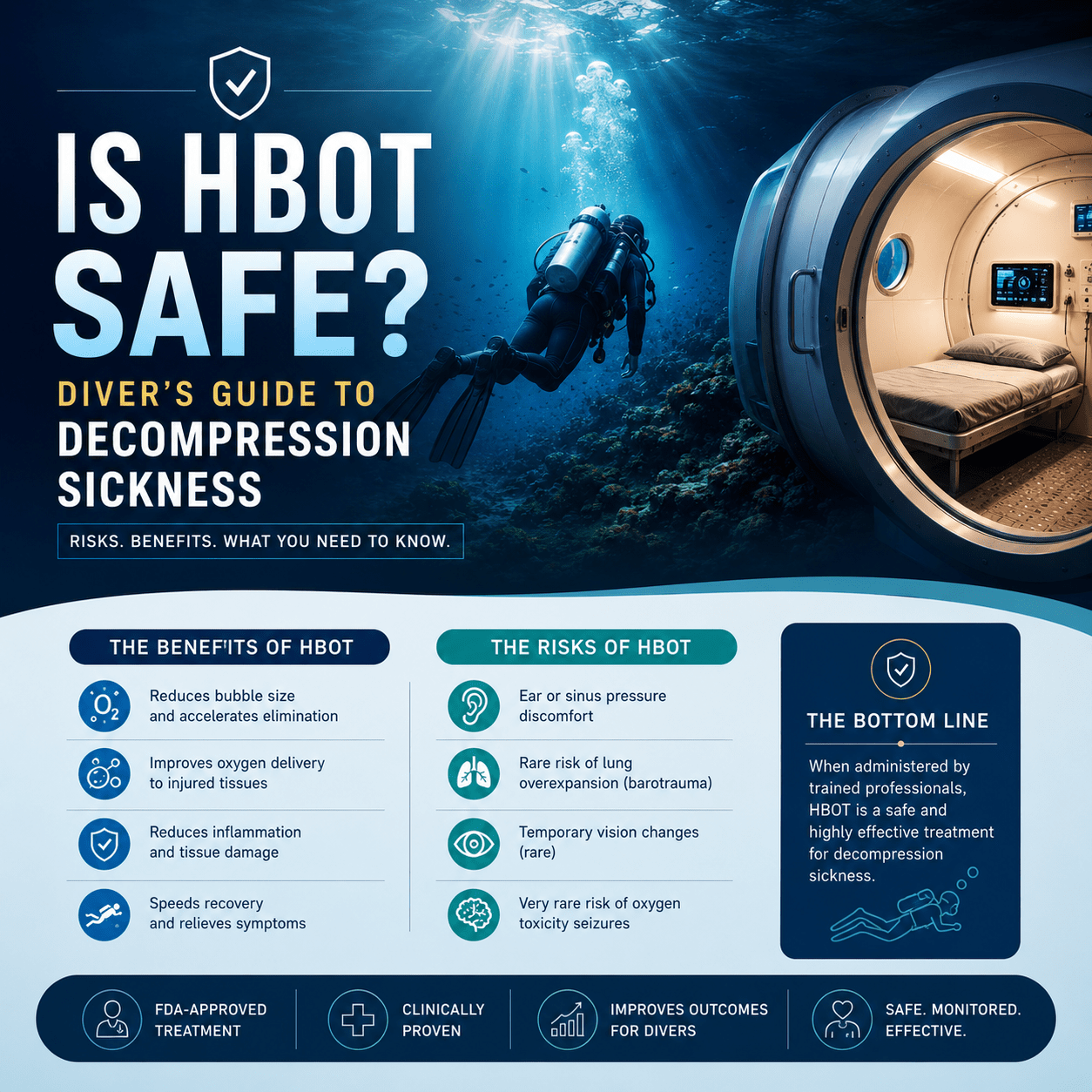
- Ear barotrauma — the most common side effect; identical sensation to aircraft descent. Resolved with equalisation. Affects approximately 2% of sessions.
- Sinus discomfort — more common in patients with active congestion. Managed with decongestants before sessions.
- Temporary myopia — mild visual changes during extended treatment courses. Fully reversible after treatment ends.
- Fatigue after early sessions — normal physiological adjustment to increased oxygen. Resolves within the first week of treatment.
| The One Serious Risk — Oxygen Toxicity | Oxygen toxicity seizures are the most feared complication of the therapy — but the numbers contextualise them correctly. At 2.0 to 2.8 ATA with standard air breaks built into protocols, the seizure rate is approximately 1 in 10,000 sessions. Seizures in the hyperbaric environment are not harmful — the patient is supine, monitored, and the oxygen is immediately reduced. No residual neurological damage has been documented from HBOT-induced oxygen toxicity seizures. |
Is HBOT Safe for Divers? Diver-Specific Considerations
Divers receiving HBOT for decompression sickness are a specific patient population with specific physiological considerations. The question is not just whether HBOT is safe in general — but whether it is safe for a diver who may have residual nitrogen load, pulmonary complications, or cardiac pathology.
Residual Nitrogen and Re-Pressurisation
A common concern among divers is whether entering a hyperbaric chamber after a DCS event worsens the nitrogen situation. The answer is no — and the mechanism is the opposite.
US Navy Treatment Tables are designed to first compress existing nitrogen bubbles through increased pressure, then gradually eliminate dissolved nitrogen during controlled decompression within the protocol. The chamber does not add more nitrogen — the patient breathes 100% oxygen, not compressed air. Nitrogen washout is accelerated, not worsened.
Pulmonary Barotrauma and Pre-Existing Lung Conditions
Divers with a history of pulmonary barotrauma — lung overexpansion during ascent — require chest assessment before HBOT. Pneumothorax is the primary absolute contraindication for HBOT and must be excluded or drained before chamber entry. For divers presenting with arterial gas embolism alongside DCS, the treating team assesses pulmonary status as a standard pre-treatment step.
Patent Foramen Ovale
Approximately 25% of the general population has a patent foramen ovale (PFO) — a small opening between the heart’s upper chambers. PFO is associated with paradoxical arterial gas embolism in divers, where venous nitrogen bubbles cross into the arterial circulation. For DCS management, the presence of PFO changes the risk assessment for future diving — but does not affect HBOT treatment safety or efficacy.
| Safety Question | Answer | Clinical Note |
| Can I enter a chamber with DCS symptoms? | Yes — this is what HBOT is for. Delay worsens outcomes. | Initiate HBOT as soon as possible after DCS diagnosis |
| Is HBOT safe with suspected pulmonary barotrauma? | Pneumothorax must be excluded first — absolute contraindication | Chest X-ray standard before HBOT if lung overexpansion suspected |
| What if symptoms improve before reaching a chamber? | Treat anyway — symptom improvement does not mean bubble resolution | Residual bubbles cause long-term damage without HBOT |
| Can I dive again after HBOT for DCS? | Not until formally cleared by a dive medicine physician | Premature return to diving risks recurrence and additional injury |
| Is HBOT safe for elderly divers? | Yes — age-adjusted monitoring for cardiac and pulmonary status | Older divers may need additional cardiovascular assessment pre-HBOT |
The Real Safety Risk for Divers Is Not HBOT — It Is Delay
Every DCS-related neurological outcome that results in permanent disability was preceded by the same event: inadequate or delayed HBOT. This is the safety message that matters most for divers.
What Happens When HBOT Is Delayed
Nitrogen bubbles in the vascular system do not simply dissolve. They migrate, coalesce, and trigger inflammatory cascades that cause secondary tissue damage beyond the initial mechanical obstruction. documented that each hour without HBOT after DCS onset allows progressive inflammatory and ischaemic injury to accumulate — injury that remains even after bubbles are eventually resolved.
Clinical outcome data is consistent: DCS patients treated within 6 hours have significantly higher rates of full neurological recovery than those treated after 24 hours. The therapy is the same. The chamber pressure is the same. The only variable is time.
First Aid That Changes Outcomes
While waiting for HBOT access, two first aid measures have documented benefit for DCS:
- 100% surface oxygen by non-rebreather mask — accelerates nitrogen elimination from blood plasma before chamber pressurisation; reduces bubble load and symptom severity
- Intravenous hydration — optimises plasma volume and circulation; supports nitrogen washout and reduces bubble aggregation
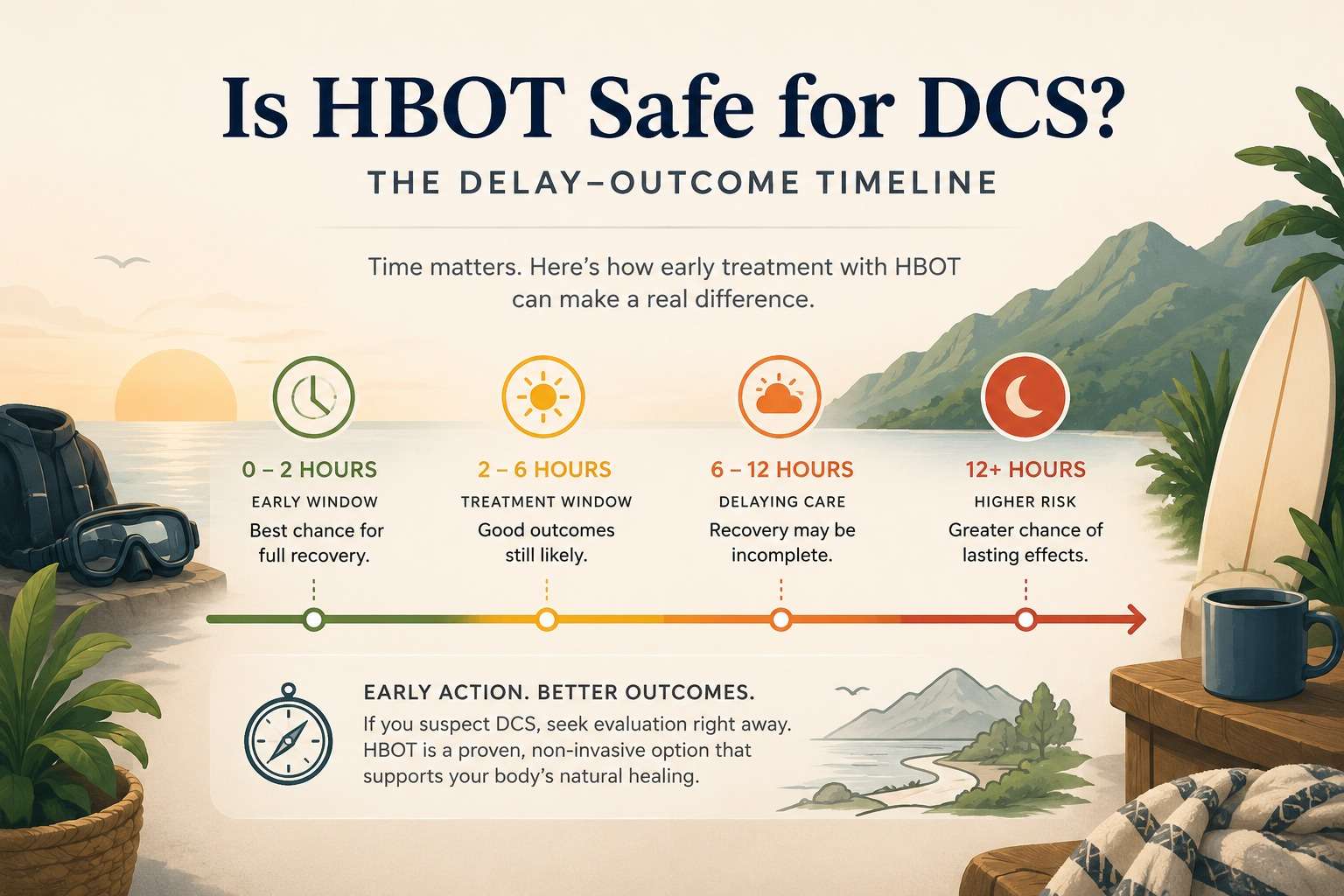
is hbot safe — DCS delay outcome timeline decompression sickness treatment window
Accessing HBOT Safely in India — What Divers Need to Know
India’s recreational and professional diving community is growing — with significant diving activity in the Andaman Islands, Lakshadweep, Goa, and along the Kerala and Tamil Nadu coasts. Yet hyperbaric facilities accessible within a safe transport time of most Indian dive sites remain limited.
The critical pre-dive checklist for Indian divers includes knowing the nearest chamber location, transport time, and contact protocol before entering the water. Emergency recompression delayed by confusion about where to go compounds every hour of delay.
For HBOT facility locations in India, see our guides to HBOT in Delhi and HBOT in Bangalore. For a comprehensive national guide to finding qualified HBOT providers, see our HBOT near me India guide.
For information on how long HBOT results take and what to expect from treatment, see our guide on how long HBOT results take.
Frequently Asked Questions
Is HBOT safe during pregnancy?
Hyperbaric therapy in pregnancy is a relative contraindication — it is not absolutely forbidden but requires careful benefit-risk assessment. For life-threatening DCS in a pregnant diver, the risk of untreated DCS to both mother and foetus outweighs the theoretical risks of HBOT. The treating dive medicine physician should make this assessment. Elective or wellness hyperbaric sessions should be deferred until after delivery.
Is HBOT safe for people with heart conditions?
Most cardiac conditions are compatible with HBOT. The therapy causes mild vasoconstriction which reduces cardiac preload — this is beneficial for most patients. Specific conditions requiring pre-treatment assessment include uncontrolled hypertension, severe heart failure, and recent myocardial infarction. A cardiologist and HBOT physician should review candidacy together for patients with significant cardiac history.
How many HBOT sessions are safe to have in total?
There is no absolute upper limit on total HBOT sessions that has been established in the literature. Extended courses — 40 sessions or more — are associated with temporary myopia in some patients and theoretical cataract progression, both of which are reversible or manageable. For DCS, the typical treatment is 1 to 3 sessions per episode. The safety profile for extended wellness or rehabilitation courses is well-established.
Is HBOT safe for children who get DCS?
Yes. Paediatric hyperbaric treatment is safe and used routinely. Children can experience DCS from breath-hold diving and, rarely, from supervised scuba training. The same US Navy Treatment Tables used for adults are applied to paediatric patients with weight-appropriate monitoring. A parent or guardian can accompany younger children in a multiplace chamber.
What should I do immediately after a dive if I suspect DCS?
- Stop diving immediately — do not re-enter the water
- Breathe 100% oxygen by non-rebreather mask continuously if available
- Stay horizontal — do not stand or exert
- Hydrate with water — not alcohol
- Contact emergency services or the nearest hyperbaric facility immediately
- Do not wait for symptoms to improve — treat as DCS until proven otherwise
HBOT Is Safe. The Delay Is Not.
The safety record of hyperbaric oxygen therapy across six decades and millions of sessions is unambiguous. Serious adverse events are rare. Side effects are mild and manageable. The therapy is well-tolerated across all ages and most medical conditions.
For divers, the safety conversation has a second chapter that matters more than the first: what happens to outcome when HBOT is delayed. The nitrogen bubble does not wait. The inflammatory cascade does not pause. The neurological damage accumulates with every hour.
Know where your nearest chamber is before the dive. Carry a non-rebreather mask. Know the symptoms. And if there is any doubt — treat as DCS and get to a chamber.
For the complete decompression sickness treatment protocol and evidence, visit our guide on decompression sickness HBOT treatment. For the full HBOT safety guide including contraindications, see our HBOT safety and risks reference.
HBOT is safe. The question every diver should ask is not whether to use it — but whether they can reach it in time.




