
Hyperbaric Oxygen Therapy Pressure: 1.3 vs 2.0 ATA Explained
“Pressure is not a setting you choose for comfort. It is the variable that determines whether HBOT works at all. The hyperbaric oxygen therapy pressure level you choose determines everything about what happens inside your body”

hyperbaric oxygen therapy pressure explained — 1.3 ATA vs 2.0 ATA plasma oxygen dissolution India
You have seen two facilities. Both offer HBOT. One charges ₹1,200 per session. One charges ₹4,500. Both use the word hyperbaric.
Someone tells you the cheaper one runs at 1.3 ATA and the more expensive one at 2.0 ATA. You ask what the difference is. Nobody gives you a straight answer.
Here is the straight answer. It is not complicated. But it changes everything about how you evaluate what you are being offered.
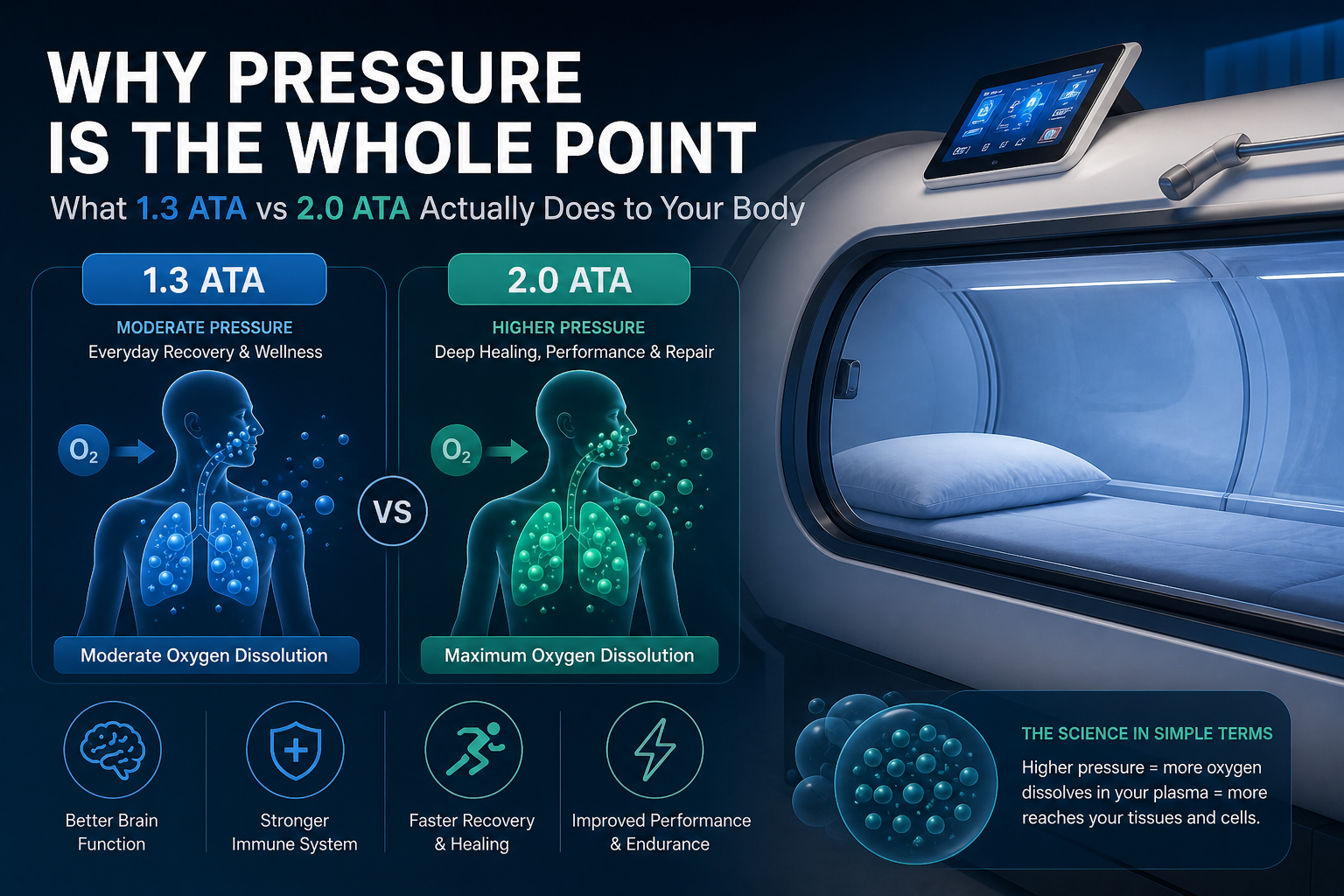
“At 1.3 ATA, your plasma carries roughly 0.6 ml of dissolved oxygen per 100 ml of blood. At 2.0 ATA breathing pure oxygen, it carries 4.4 ml. That is not a marginal difference. That is a 7-fold increase in the oxygen available to your tissues.”
Hyperbaric Oxygen Therapy Pressure — Why It Is the Whole Mechanism
HBOT stands for Hyperbaric Oxygen Therapy. Hyperbaric means above normal atmospheric pressure. That word — hyperbaric — is not a brand description. It is a physical specification. Without genuine pressure elevation, you are not doing hyperbaric therapy. You are sitting in an inflated tent breathing slightly enriched air.
Henry’s Law — The Science in One Sentence
Henry’s Law states that the amount of a gas dissolved in a liquid is proportional to the partial pressure of that gas above the liquid. Applied to HBOT: the more pressure you apply, the more oxygen dissolves directly into your blood plasma.
| Henry’s Law Applied | At 1.0 ATA (normal atmosphere) breathing air: plasma carries 0.3 ml O₂ per 100 ml blood. At 2.0 ATA breathing 100% pure oxygen: plasma carries 4.4 ml O₂ per 100 ml blood. This plasma-dissolved oxygen travels independently of red blood cells — reaching tissues that normal circulation cannot adequately supply. Thom SR (Plastic and Reconstructive Surgery, 2011) identified this plasma dissolution as the primary driver of HBOT’s therapeutic mechanism. |
Why Plasma Dissolution Matters
Under normal conditions, approximately 98% of oxygen in your blood travels via haemoglobin in red blood cells. Red blood cells are already saturated at sea level — breathing more oxygen at normal pressure adds negligible additional oxygen to your blood.
Pressure changes this entirely. When you increase atmospheric pressure while breathing pure oxygen, Henry’s Law forces additional oxygen to dissolve directly into plasma — the liquid component of blood that can penetrate tissues red blood cells cannot reach. Gill and Bell (QJM: An International Journal of Medicine, 2004) documented this mechanism comprehensively: plasma-dissolved oxygen under pressure reaches hypoxic tissues through diffusion pathways unavailable to haemoglobin-bound oxygen.
This is why HBOT works for wound healing, neuroplasticity, and cellular repair. And it is why the pressure level is not a preference — it is the mechanism.
What 1.3 ATA vs 2.0 ATA Actually Delivers — The Numbers
The table below maps the five most common pressure levels in HBOT practice to their plasma oxygen delivery, biological effects, and the research that supports each level. Read it carefully — this is the information most buyers in India never see.
| Pressure Level | Plasma O₂ (ml/100ml blood) | Oxygen Delivery Mode | Biological Effect | Typical Chamber Type |
| 1.0 ATA (Normal atmosphere) | 0.3 ml | Red blood cell transport only | Standard cellular function — no therapeutic augmentation | Not applicable |
| 1.3 ATA (Low-pressure soft chamber) | ~0.6–0.9 ml | Marginal plasma dissolution begins | Mild recovery support; general wellness | Soft / inflatable chamber |
| 1.5 ATA (Mid-range) | ~1.5–2.0 ml | Modest plasma dissolution | Some anti-inflammatory effect; limited neuroplasticity | Hard chamber minimum |
| 2.0 ATA (Clinical standard) | ~4.4 ml | Significant plasma dissolution | Full therapeutic cascade: angiogenesis, stem cells, healing | Hard chamber required |
| 2.4 ATA (Upper therapeutic range) | ~6.0 ml | Maximum safe plasma dissolution | Plasma alone meets resting O₂ needs | Medical hard chamber |
The conclusion is direct: the biological cascade that drives HBOT’s documented outcomes — stem cell mobilisation, angiogenesis, neuroplasticity, wound healing acceleration, telomere effects — begins in earnest at 2.0 ATA. It does not occur to the same degree at 1.3 ATA.
This is not a commercial position. It is what the peer-reviewed research shows.
What 1.3 ATA Can Do — and What It Cannot
Low-pressure soft chamber HBOT is not worthless. It is important to be precise about what it delivers rather than dismissing it entirely.
What 1.3 ATA Can Support
- General recovery and mild fatigue — the modest elevation in available oxygen supports cellular energy production
- Accessibility and convenience — soft chambers are portable, lower cost, and suitable for home use
- Mild anti-inflammatory effect — some reduction in inflammatory markers has been observed at lower pressures
- Wellness and general oxygenation — for buyers seeking general wellbeing rather than a specific clinical outcome
What 1.3 ATA Cannot Replicate
- The Efrati longevity protocol — 38% telomere lengthening and 37% reduction in senescent cells was measured at 2.0 ATA. This result does not transfer to 1.3 ATA.
- Post-concussion and TBI neuroplasticity protocols — Boussi-Gross et al. (PLoS ONE, 2013) demonstrated improvement in post-concussion syndrome at 1.5 ATA minimum using hard chamber.
- Wound healing at clinical depth — the oxygen partial pressure required to support tissue repair in hypoxic wounds requires 2.0 ATA and pure oxygen delivery (Bhutani & Vishwanath, Indian J Plast Surg, 2012).
- Stem cell mobilisation — Thom SR et al. (American Journal of Physiology, 2006) documented stem cell mobilisation following HBOT at therapeutic pressure. Low-pressure sessions do not replicate this mechanism at the same magnitude.
The honest summary: 1.3 ATA soft chamber HBOT is a wellness tool. 2.0 ATA hard chamber HBOT is what the clinical research describes. They are not the same thing. Both are real — but they are not interchangeable.
What This Means When You Walk Into a Facility
Most HBOT buyers in India evaluate facilities on price, location, and aesthetics. Almost nobody asks the one question that determines whether the session they are paying for can produce the outcome they want.
“What pressure does your chamber reach — and can it sustain that pressure for a full 90-minute session without loss?”
A facility running a hard chamber at 2.0 ATA with pure oxygen delivery can tell you this immediately. They know it matters and they are proud of it.
A facility running a soft chamber at 1.3 ATA may describe their offering as hyperbaric therapy, HBOT, or oxygen therapy. Technically, 1.3 ATA is above atmospheric pressure — so none of those descriptions are false. But the pressure level is the variable that determines what you are actually getting.
You now have the number. Ask for it.
Still not sure what you’re being offered? If you have been given a price, a session description, or a chamber specification and you want to understand what it actually means — ask us. We will give you a straight answer with no obligation.
How to Read a Facility’s Pressure Claim
There are three things a facility can tell you about pressure — and they are not all equally meaningful.
Maximum Pressure vs Operating Pressure
A chamber may be rated to a maximum of 2.0 ATA but routinely operated at 1.5 ATA for shorter sessions. Ask what pressure the session is actually run at — not what the chamber is theoretically capable of. The outcome research specifies operating pressure, not hardware ratings.
Sustained Pressure vs Peak Pressure
Some chambers reach their rated pressure briefly but cannot sustain it for a full 90-minute session due to compressor limitations or seal quality. The relevant question is not “does it reach 2.0 ATA” but “does it sustain 2.0 ATA for 90 minutes without pressure bleed.” A chamber that peaks at 2.0 ATA and drops to 1.6 ATA within 20 minutes is not delivering a 2.0 ATA session.
Pressure With Pure Oxygen vs Pressure With Ambient Air
As our guide to
what medical-grade HBOT chambers actually require what medical-grade HBOT chambers actually require explains, pressure alone is not sufficient. The chamber must deliver pure oxygen — not pressurised ambient air — for the plasma dissolution mechanism to occur at therapeutic levels. A chamber pressurising with air at 2.0 ATA delivers a fraction of the therapeutic oxygen partial pressure of a chamber delivering 100% O₂ at the same pressure.
Frequently Asked Questions
1. Does 1.3 ATA HBOT have any value at all?
2. What is the maximum safe pressure for HBOT?
3. Can I get the same results with more sessions at lower pressure?
4. How do I know if the facility near me is running at 2.0 ATA?
5. Does pressure affect safety, not just effectiveness?
Pressure Is Not a Detail. It Is the Whole Point.
Every significant finding in HBOT research — the neuroplasticity outcomes, the longevity data, the wound healing protocols, the stroke recovery evidence — was produced at a specific pressure. That pressure was chosen because the biology requires it.
1.3 ATA is above atmospheric. It is technically hyperbaric. But the outcomes associated with clinical HBOT research are not produced at 1.3 ATA.
2.0 ATA with pure oxygen delivery is where the mechanism activates at therapeutic levels. You now know why. You now know what to ask.
For the full picture of what makes a chamber capable of delivering that pressure reliably and safely, read our guide to what a medical-grade HBOT chamber actually requires.
For how HBOT works at a cellular level once that pressure is reached, see how HBOT works inside the body.
Have a specific question about what you’ve been offered? If you’re evaluating a facility, comparing a quote, or trying to understand whether the chamber you’ve been shown can deliver the protocol you need — we’re here to help you think it through.



4 Comments
Comments are closed.


[…] 1.3 ATA versus 2.0 ATA actually delivers what 1.3 ATA versus 2.0 ATA actually delivers explains, the difference between these two pressure levels is not marginal. It determines whether […]
[…] pressure determines HBOT outcomes why pressure determines HBOT outcomes explains, the therapeutic cascade requires 100% oxygen at 2.0 ATA. Ambient air at any pressure […]
[…] For the biology behind why each pressure threshold matters — why 1.5 ATA and 2.0 ATA produce different outcomes — see our detailed guide to hyperbaric oxygen therapy pressure explained. […]
[…] For the pressure science that explains why category differences matter biologically, read our guide to why 1.3 ATA and 2.0 ATA produce different outcomes. […]