
Hyperbaric Oxygen Therapy Pressure: Why 2.5 ATA Is What Carbon Monoxide Poisoning Requires
Standard oxygen therapy runs at 1 atmosphere. At that pressure, CO half-life in blood is 60 to 90 minutes. At 2.5 ATA, it falls to 20 minutes. The pressure is not a setting preference. It is the treatment.
 hyperbaric oxygen therapy pressure CO poisoning — 2.5 ATA treatment carbon monoxide brain protection
hyperbaric oxygen therapy pressure CO poisoning — 2.5 ATA treatment carbon monoxide brain protection
Hyperbaric oxygen therapy pressure is not a technical detail. For carbon monoxide poisoning, it is the entire mechanism.
Standard oxygen therapy — the 100% oxygen mask given in every emergency room — is effective. It reduces CO half-life in blood from five hours (breathing room air) to 60 to 90 minutes. For mild CO exposure, this is often sufficient.
But for serious CO poisoning, two problems remain that normal atmospheric pressure cannot address. First, CO bound to mitochondrial cytochrome c oxidase — the enzyme that produces cellular energy — is not cleared by normal pressure oxygen. Second, the delayed neurological syndrome that affects up to 30% of serious CO poisoning survivors develops from this mitochondrial injury, not from CO in the blood.
Hyperbaric oxygen therapy at 2.5 ATA addresses both. The pressure is the difference between treating symptoms and treating the cause.
For the full clinical evidence and treatment protocol, see our guide on carbon monoxide poisoning and HBOT brain protection. For the foundational mechanism behind how pressure changes oxygen delivery, visit How HBOT Works.
Hyperbaric oxygen therapy pressure: The atmospheric pressure inside the chamber during an HBOT session, expressed in atmospheres absolute (ATA). Standard atmospheric pressure is 1.0 ATA. For carbon monoxide poisoning, the standard treatment pressure is 2.5 ATA — creating plasma oxygen concentrations that displace CO from mitochondrial binding sites that normal atmospheric pressure cannot reach.
Why Hyperbaric Oxygen Therapy Pressure Changes CO Outcomes
To understand why pressure matters in CO poisoning, you need to understand what CO actually does — and why haemoglobin is only part of the problem.
What CO Does — The Two-Level Attack
Carbon monoxide binds to haemoglobin with 250 times the affinity of oxygen — displacing it from the carrier molecule and reducing blood’s oxygen-carrying capacity dramatically. This is the mechanism most people know: CO causes oxygen deficiency by blocking haemoglobin.
But CO also binds to cytochrome c oxidase — the terminal enzyme in the mitochondrial electron transport chain, responsible for producing ATP in every cell in the body. This mitochondrial binding is independent of haemoglobin. It persists after CO has been cleared from the blood. And it is the mechanism behind the delayed neurological syndrome (DNS) that develops days to weeks after CO poisoning — often in patients who appeared to fully recover initially.
The mitochondrial mechanism was documented by — confirming that CO’s binding to cytochrome c oxidase disrupts cellular energy production in a way that continues causing neurological damage long after the patient’s blood CO level has normalised.
Why Standard Oxygen Pressure Cannot Reach Mitochondrial CO
At 1.0 ATA, breathing 100% oxygen clears CO from haemoglobin in 60 to 90 minutes. But the partial pressure of oxygen at 1.0 ATA is not sufficient to displace CO from cytochrome c oxidase. The binding affinity of CO to the mitochondrial enzyme is different from its affinity to haemoglobin — and the displacement requires a higher oxygen concentration than standard atmospheric pressure can achieve.
This is the therapeutic gap that hyperbaric oxygen therapy pressure closes.
| Treatment | Pressure | CO Half-Life (Blood) | Mitochondrial CO Cleared? | DNS Prevention? |
| Breathing room air | 1.0 ATA (21% O₂) | ~5 hours | No | No |
| Standard O₂ mask | 1.0 ATA (100% O₂) | 60–90 minutes | No | Partial |
| Hyperbaric O₂ at 2.5 ATA | 2.5 ATA (100% O₂) | ~20 minutes | Yes | Yes — documented |
The half-life of CO in blood drops from 5 hours to 20 minutes at 2.5 ATA. That is a 15-fold acceleration. But the more important difference is at the mitochondrial level — where only the higher oxygen partial pressure at 2.5 ATA can displace CO from cytochrome c oxidase and prevent DNS.
What Hyperbaric Oxygen Therapy Pressure of 2.5 ATA Achieves in the Brain
The brain is the organ most affected by CO poisoning — and the organ for which the pressure of 2.5 ATA is most critical. Here is what happens at each treatment level.
Haemoglobin CO Clearance — Faster at Every Pressure
At 2.5 ATA, the massively increased partial pressure of oxygen creates a competitive displacement environment for CO on haemoglobin. The reaction that normally takes 60 to 90 minutes at normal atmospheric pressure completes in approximately 20 minutes. This rapid clearance reduces the total CO load on tissue before secondary inflammatory cascades can establish.
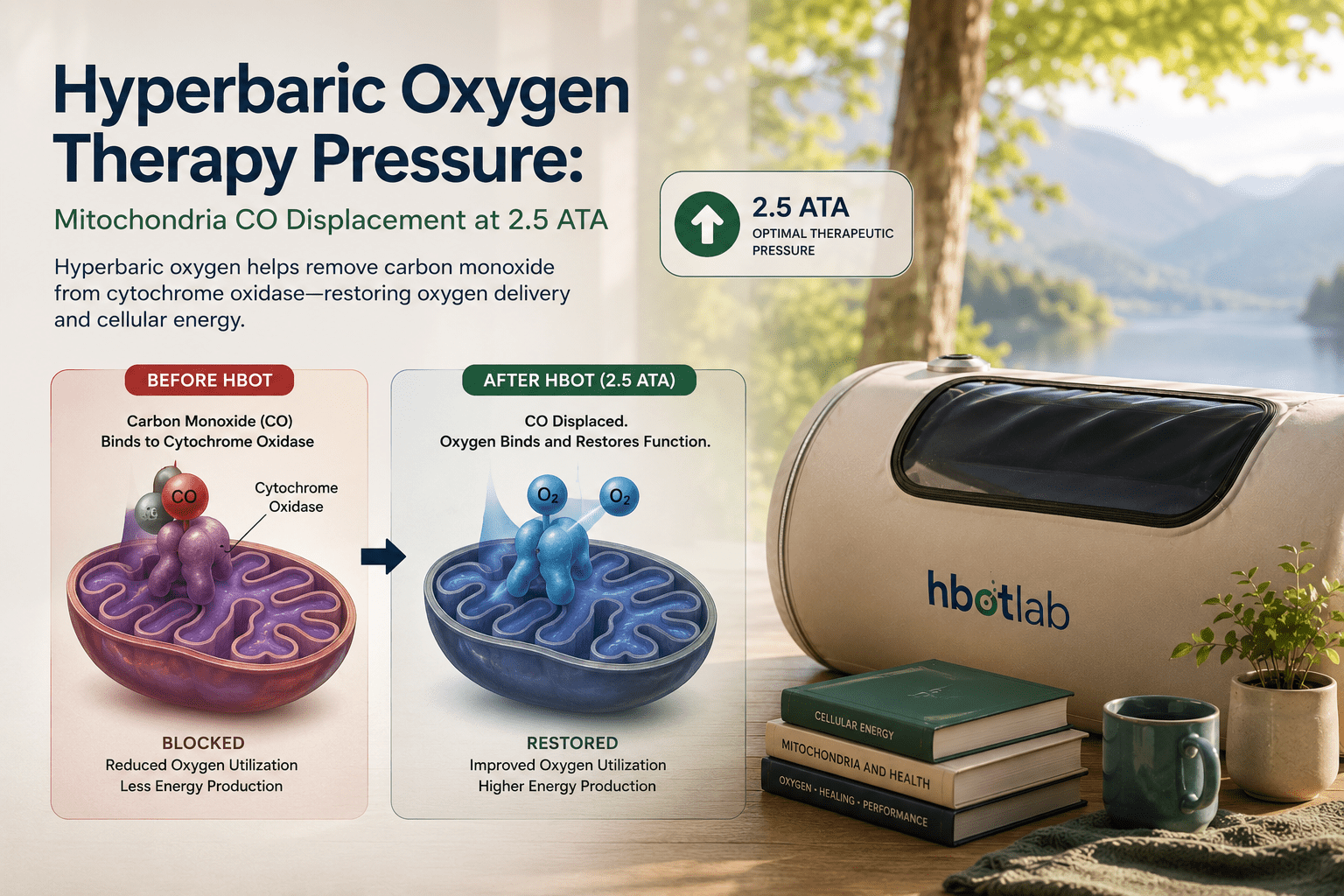
Mitochondrial CO Displacement — Only at Elevated Pressure
At 2.5 ATA, plasma oxygen concentrations reach levels that successfully compete with CO for cytochrome c oxidase binding — displacing CO from the mitochondrial enzyme and restoring cellular energy production. confirmed that HBOT at therapeutic pressure restores mitochondrial membrane function and ATP synthesis in CO-poisoned tissue — the mechanism that standard oxygen therapy cannot replicate regardless of how long it is administered.
Neuroinflammation Reduction
CO poisoning triggers a neuroinflammatory cascade — leukocyte activation, oxidative damage, and microvascular injury in brain tissue — that continues after CO clearance. documented that HBOT at therapeutic pressure modulates this neuroinflammatory response, reducing neutrophil-endothelium adhesion and limiting the secondary brain injury that outlasts the initial CO exposure.
DNS Prevention — The Clinical Outcome That Justifies the Pressure
Delayed neurological syndrome affects 10 to 30% of serious CO poisoning survivors who receive only standard oxygen treatment. — a landmark randomised controlled trial — documented that HBOT at 2.5 ATA significantly reduced the incidence of cognitive sequelae at 6 weeks and 12 months compared to normobaric oxygen. The pressure-dependent mitochondrial protection mechanism is what makes this difference possible.
hyperbaric oxygen therapy pressure — mitochondria CO displacement 2.5 ATA cytochrome oxidase
Who Requires Full Hyperbaric Oxygen Therapy Pressure — Clinical Criteria
Not every CO poisoning patient requires HBOT at 2.5 ATA. The pressure and the intervention are indicated when the risk of DNS or serious neurological outcomes is elevated. The clinical criteria are well-established.
Absolute Indications for HBOT at 2.5 ATA
- Loss of consciousness at any point — even transient loss indicates severe CO exposure with high DNS risk
- Neurological symptoms at presentation — confusion, altered consciousness, focal deficits, seizures
- COHb > 25% at presentation — blood CO level indicating severe exposure
- Pregnancy — foetal haemoglobin binds CO more tightly; foetal risk is disproportionately high at lower maternal exposure levels
- Cardiac involvement — chest pain, ECG changes, elevated troponin — CO damages cardiac mitochondria independently
Strong Relative Indications
- Age over 36 years — independent risk factor for DNS regardless of symptom severity
- Metabolic acidosis — pH <7.1 indicates significant tissue hypoxia from CO
- Prolonged exposure (closed space > 4 hours) — duration of exposure predicts mitochondrial CO burden
| India Context | CO poisoning from generator exhaust, gas heaters, coal fires, and kerosene stoves represents a significant preventable mortality burden in India — particularly in winter months in North India and during power outage events. Awareness among Indian emergency physicians that HBOT at 2.5 ATA prevents DNS — not just treats acute symptoms — remains extremely low. Most Indian emergency departments treat CO poisoning with normobaric oxygen alone. |
Accessing Hyperbaric Oxygen Therapy at the Right Pressure in India
The critical variable in CO poisoning outcomes is time to HBOT — and in India, most emergency departments are not co-located with a hyperbaric facility. Normobaric oxygen should be initiated immediately in any emergency department while transport to a hyperbaric centre is arranged. The two interventions are not mutually exclusive — normobaric oxygen continues during transport, and HBOT begins as soon as the patient reaches the chamber.
For HBOT facility locations in India, see our guides to HBOT in Delhi and HBOT in Bangalore. For a complete national facilities guide, visit our HBOT near me India guide.
For the complete CO poisoning treatment protocol and evidence, see our guide on carbon monoxide poisoning and HBOT brain protection.
Frequently Asked Questions
Why is 2.5 ATA used for CO poisoning and not a higher pressure?
2.5 ATA achieves the plasma oxygen concentrations required to displace CO from cytochrome c oxidase while maintaining an acceptable oxygen toxicity risk profile. Higher pressures — 3.0 ATA and above — produce marginally faster CO clearance but significantly higher oxygen toxicity risk, particularly central nervous system seizures. The benefit-risk calculation at 2.5 ATA is optimal for CO poisoning. Higher pressures are reserved for decompression sickness and arterial gas embolism, where bubble compression physics require them.
How long does an HBOT session last for CO poisoning?
The standard protocol is 90 minutes at 2.5 ATA, with air breaks to prevent oxygen toxicity. Serious cases may receive two to three sessions in the first 24 hours. The number of sessions is determined by symptom severity, neurological status, and clinical response. Patients who present with loss of consciousness typically receive a minimum of three sessions regardless of apparent recovery.
If I feel better after normobaric oxygen, do I still need HBOT?
Yes — in cases meeting the clinical criteria above. Symptom improvement with normobaric oxygen reflects haemoglobin CO clearance, not mitochondrial CO clearance. DNS develops from mitochondrial injury, not haemoglobin CO, and can present days to weeks after apparently full recovery. Feeling better is not the same as being protected from DNS. Clinical assessment by an emergency physician determines whether HBOT is indicated regardless of symptomatic improvement.
Can HBOT be used for mild CO poisoning?
For mild CO poisoning without loss of consciousness, significant neurological symptoms, or the clinical criteria listed above, normobaric oxygen is generally sufficient. HBOT is reserved for presentations where DNS risk is elevated. The decision is clinical — made by the treating physician based on symptom severity, exposure duration, COHb level, and patient-specific factors including age and pregnancy.
What is the CO poisoning protocol used at Indian HBOT centres?
Most Indian hospital-based hyperbaric units follow the US Navy/UHMS protocol: 2.5 ATA for 90 minutes with air breaks, repeated for 2 to 3 sessions in serious cases. Some centres use the Weaver protocol — 2.4 ATA — derived from the landmark 2002 randomised controlled trial. Both protocols produce equivalent outcomes. The key variable is time to treatment, not the specific pressure variant used.
The Pressure Is Not Incidental. It Is the Treatment.
Standard oxygen therapy does the first job — clearing CO from haemoglobin and restoring blood oxygen-carrying capacity. It does this well, and in mild CO poisoning it is sufficient.
The second job — clearing CO from mitochondria, preventing DNS, protecting neurological function — requires the elevated partial pressure that only hyperbaric oxygen therapy delivers. Not as a supplement to standard treatment. As the mechanism that standard treatment physically cannot replicate.
The number 2.5 ATA is not arbitrary. It is the pressure at which plasma oxygen concentrations reach the level required to displace CO from cytochrome c oxidase. Understanding why that pressure matters is understanding why delayed neurological syndrome is preventable — and why families of CO poisoning patients should ask about HBOT before the window for DNS prevention closes.
For the complete CO poisoning treatment evidence, see our guide on carbon monoxide poisoning and HBOT brain protection. For the full conditions evidence base, explore our HBOT conditions section.
The pressure clears the CO that standard oxygen leaves behind. That is what saves neurological function.




