
When Blood Flow Stops: HBOT as the Bridge Between Vascular Crisis and Tissue Survival
When Blood Flow Stops: HBOT as the Bridge Between Vascular Crisis and Tissue Survival
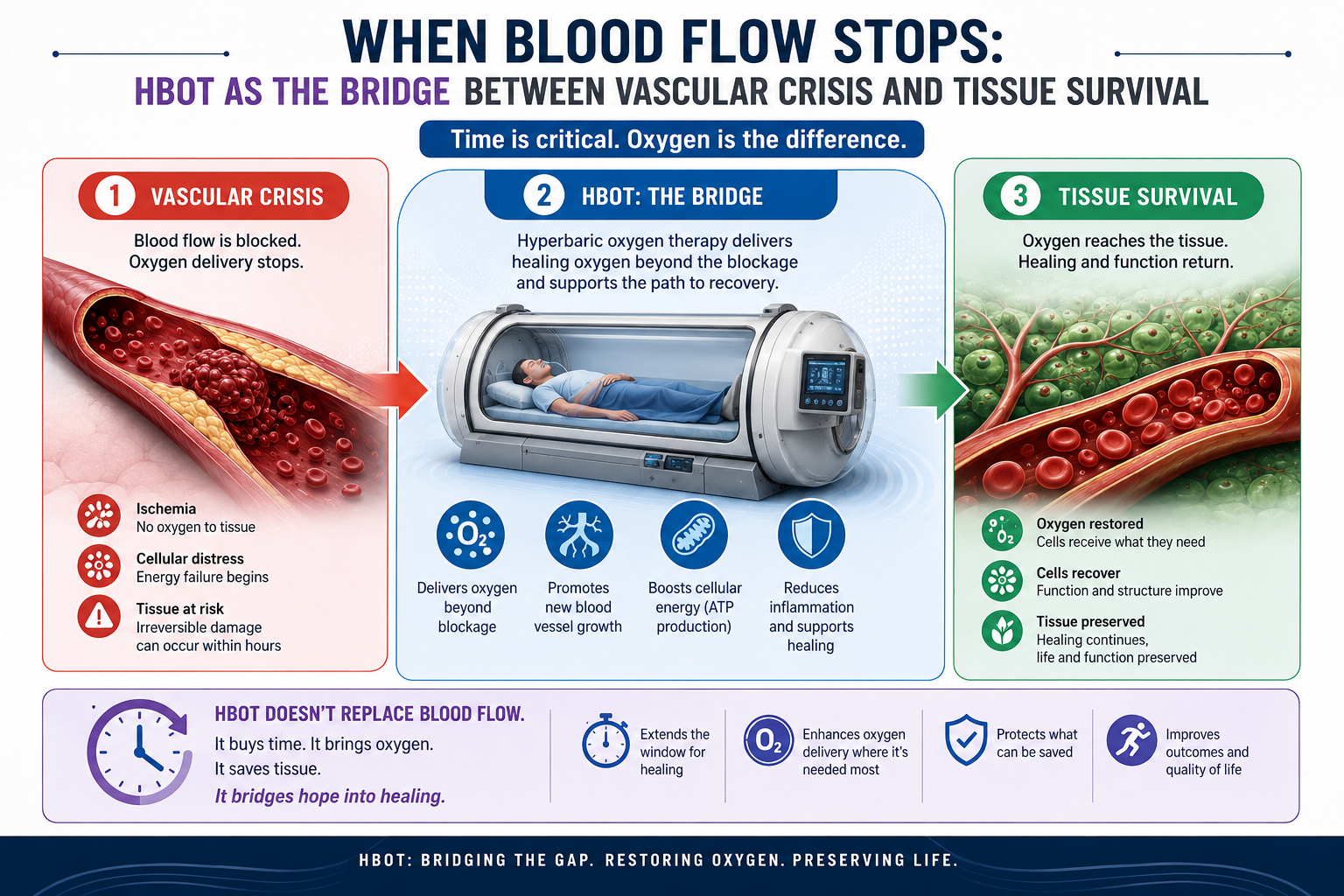
HBOT cannot unblock an artery. But it can keep tissue alive until surgery can. At 2.0 ATA, plasma-dissolved oxygen reaches ischaemic tissue through diffusion alone — without needing blood flow at all.
HBOT acute arterial insufficiency treatment — hyperbaric oxygen therapy vascular crisis tissue survival
When an artery is blocked, the tissue it feeds begins to die. Every minute matters.
This is acute arterial insufficiency — the sudden loss of blood flow to tissue that depends on it for survival. Whether it happens in a limb, a retinal artery, or any other end-organ, the biology is the same: oxygen delivery stops, cells begin to fail, and the window between reversible and irreversible damage closes with every minute that passes.
Surgery is the definitive answer. A blocked artery needs to be unblocked — through embolectomy, bypass, or endovascular intervention. HBOT cannot do this. That is not its role.
HBOT’s role is the window between blockage and repair. It is the bridge therapy — the intervention that keeps tissue viable in the hours when surgery is being arranged, when the anatomy is being assessed, when the anaesthetist is being called. It delivers oxygen to ischaemic tissue through a mechanism that does not require blood flow at all.
Understanding this mechanism — and why it changes outcomes when deployed early — is what this article is about.
For a complete explanation of how HBOT delivers oxygen under pressure, visit How HBOT Works.
What Acute Arterial Insufficiency Is — and Why It Is an Emergency
Acute arterial insufficiency describes the sudden, severe reduction in blood supply to tissue — insufficient to meet the metabolic needs of that tissue. It is distinct from chronic arterial disease, where reduced flow develops gradually and collateral vessels compensate over time. In acute insufficiency, the reduction is abrupt. There is no time for collateral development. The tissue is simply cut off.
Common Causes
- Acute arterial embolism — a clot travelling from the heart or a proximal vessel and lodging in a peripheral artery
- Acute arterial thrombosis — in-situ clot formation at a site of pre-existing atherosclerotic disease
- Traumatic arterial injury — from crush injury, penetrating trauma, or iatrogenic vascular damage
- Compartment syndrome — where rising pressure within a closed fascial compartment compresses arterial inflow
- Post-surgical vascular compromise — following bypass procedures, grafts, or reconstructive surgery
- Central retinal artery occlusion — the ophthalmic emergency where the artery supplying the retina is suddenly blocked
The Ischaemia Clock
The severity of tissue damage in acute arterial insufficiency is directly proportional to the duration of ischaemia. Different tissues have different tolerances — but all have limits.
| Tissue Type | Tolerance to Warm Ischaemia | Clinical Implication |
|---|---|---|
| Skeletal muscle | 4–6 hours before irreversible necrosis | Standard limb salvage window — primary surgical target |
| Peripheral nerve | 2–4 hours before permanent dysfunction | Neurological deficits can persist even after revascularisation |
| Retina | 60–90 minutes for complete irreversible loss | CRAO: the narrowest treatment window in vascular medicine |
| Skin / subcutaneous tissue | 8–12 hours | More tolerant — but still affected by prolonged ischaemia |
| Myocardium | 20–40 minutes before irreversible damage | Cardiac surgical emergency — separate protocol |
| Brain tissue | 4–6 minutes | Stroke — separate protocol; most time-sensitive organ |
The retinal artery has the narrowest ischaemia window in vascular medicine — 60 to 90 minutes before permanent vision loss. Central retinal artery occlusion is an ophthalmic emergency. HBOT is the only documented intervention that can reverse retinal ischaemia within this window.
How HBOT Keeps Tissue Alive Without Blood Flow — The Physics
This is the mechanism that makes HBOT uniquely valuable in acute arterial insufficiency. And it is grounded in straightforward physics — Henry’s Law, applied clinically.
1. Normal Oxygen Delivery — The Haemoglobin Dependency
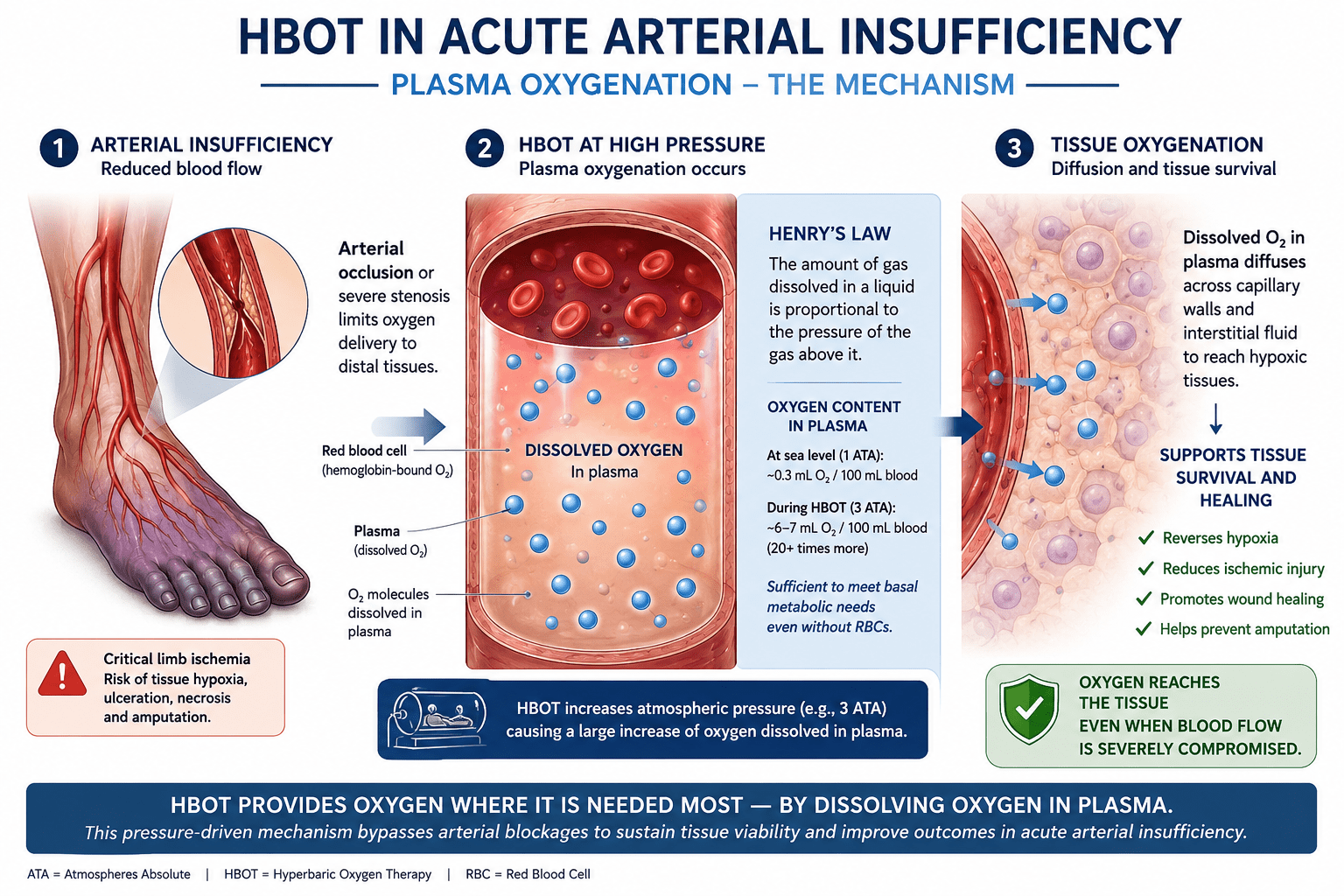
Under normal conditions, red blood cells carry 98% of the oxygen in blood. Plasma — the liquid portion — carries approximately 0.3 ml of oxygen per 100 ml of blood. This is insufficient to sustain tissue at rest, which requires approximately 6 ml O₂ per 100 ml blood. Without red blood cells moving through functioning arteries, tissue starves.
This is why arterial blockage is so immediately dangerous. The oxygen carrier system is stopped at the artery. Tissue downstream receives neither the carrier nor the oxygen.
2. HBOT — Bypassing the Need for Blood Flow
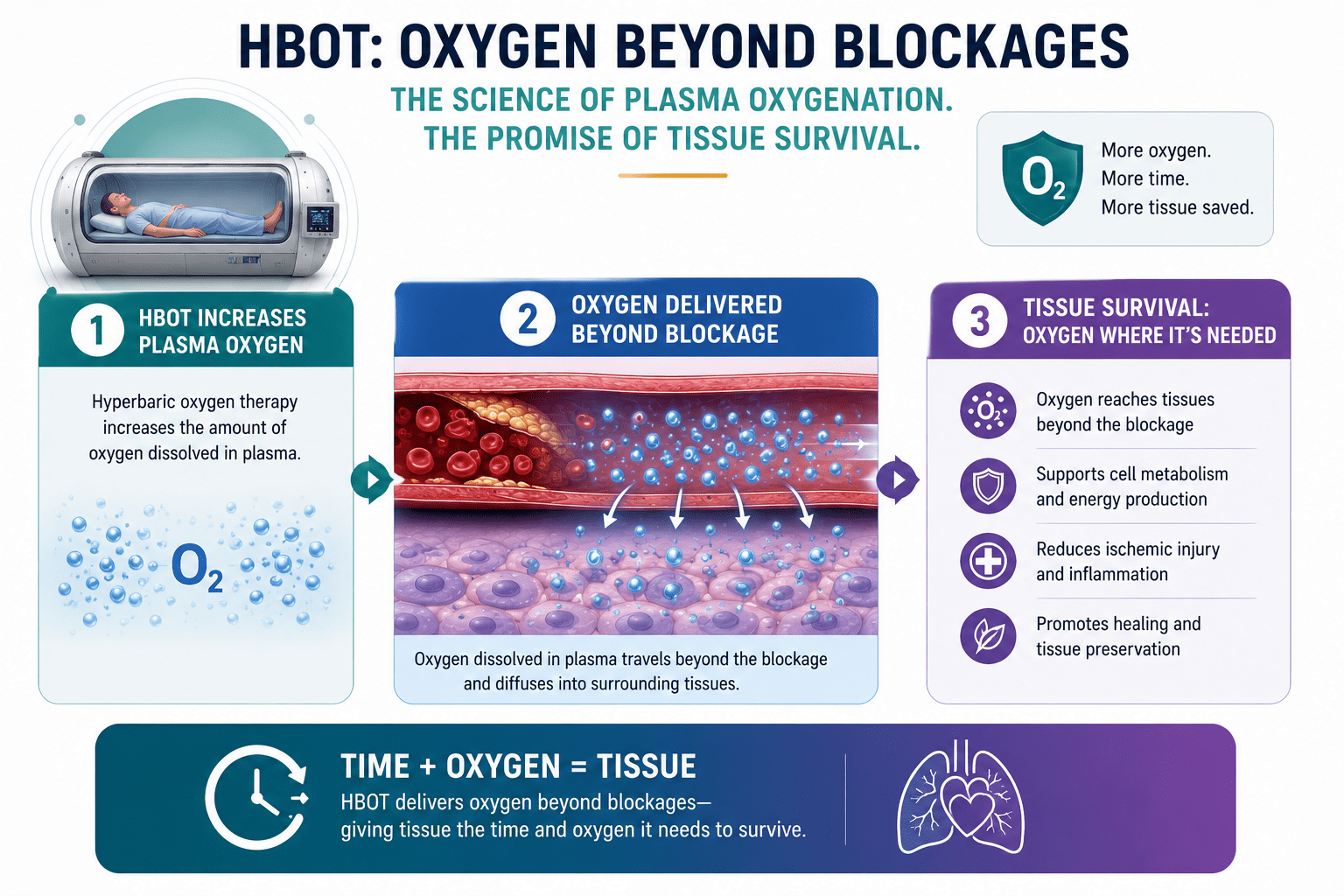
Henry’s Law states that the amount of gas dissolved in a liquid is proportional to the partial pressure of that gas above the liquid. At 2.0 ATA, the partial pressure of oxygen breathed at 100% concentration rises dramatically — and dissolved oxygen in plasma increases approximately 20-fold compared to breathing normal air at sea level. documented that plasma-dissolved oxygen at 2.0–2.4 ATA reaches concentrations sufficient to meet resting tissue oxygen requirements without any haemoglobin contribution.
This plasma-dissolved oxygen reaches tissue through diffusion — driven by the pressure gradient between the oxygen-rich plasma and the oxygen-starved ischaemic cells. It does not need a functioning artery to travel through. It diffuses through whatever extravascular pathway exists, reaching cells that would otherwise receive nothing.
At 2.4 ATA, plasma carries approximately 6 ml O₂ per 100 ml blood — enough to meet resting tissue oxygen requirements without any haemoglobin. An artery is blocked. Oxygen still arrives. This is the bridge.
3. What Plasma Diffusion Achieves — and Its Limits
Plasma diffusion oxygenation is a bridge, not a cure. It sustains tissue at rest — preventing the cell death that accumulates during ischaemia. It does not restore normal metabolic function, does not support active tissue or exercise oxygen demands, and does not replace the need for vascular repair.
But sustaining tissue at rest through the critical window — keeping muscle fibres alive until the surgeon revascularises, keeping retinal cells viable until the chamber is reached — is precisely what changes outcomes. The tissue that survives the ischaemic window is the tissue that recovers function after revascularisation.
Three Mechanisms — Not Just Oxygenation
Mechanism 1 — Plasma Oxygenation of Ischaemic Tissue
As described above — the primary bridging mechanism. Dissolved oxygen delivered through plasma diffusion to tissue that arterial occlusion has cut off from its normal oxygen supply.
Mechanism 2 — Reduction of Reperfusion Injury
When blood flow is eventually restored — through surgery, embolectomy, or spontaneous recanalisation — ischaemic tissue is at risk of reperfusion injury: the paradoxical second wave of damage triggered by reoxygenation. documented that HBOT modulates the reactive oxygen species cascade and neutrophil-endothelium adhesion that drives reperfusion injury — protecting tissue from the inflammatory wave that restoration of flow can trigger.
This same mechanism is described in our article on HBOT for crush injury and compartment syndrome — reperfusion injury is the shared biological challenge across all ischaemia-reperfusion conditions.
Mechanism 3 — Oedema Reduction
HBOT at therapeutic pressure causes mild vasoconstriction in non-ischaemic tissue — reducing oedema in the areas surrounding the arterial occlusion. This reduces compartment pressure in closed fascial spaces, improves collateral flow to the ischaemic region, and creates a better biological environment for the tissue at risk.
and the StatPearls review on HBOT cardiovascular effects both document that hyperbaric oxygen-induced vasoconstriction reduces tissue oedema without compromising oxygen delivery — because the dramatic increase in plasma-dissolved oxygen compensates for any flow reduction.
HBOT acute arterial insufficiency — plasma oxygenation mechanism Henry’s Law tissue survival
Central Retinal Artery Occlusion — The Eye Emergency HBOT Can Reverse
Of all the conditions within acute arterial insufficiency, central retinal artery occlusion (CRAO) represents the most specific and time-critical HBOT application — and has the strongest individual case series evidence for functional recovery.
What CRAO Is
CRAO is the sudden blockage of the central retinal artery — the sole blood supply to the inner retinal layers. It presents as sudden, painless, complete or near-complete loss of vision in one eye. It is, in effect, a stroke of the eye.
Without treatment, the retina begins irreversible necrosis within 90 to 100 minutes. The inner retinal layers — the ganglion cells and nerve fibre layer — are the most sensitive to ischaemia and the first to die permanently.
Why HBOT Is the Only Documented Reversal Intervention
Standard CRAO management — intraocular pressure reduction, anterior chamber paracentesis, ocular massage — aims to dislodge the embolus. These interventions address the mechanical obstruction. They do not address the oxygen deprivation of the retinal tissue during the window when the embolus is still in place.
HBOT oxygenates the ischaemic retina through plasma diffusion — the choroidal circulation, which is not supplied by the central retinal artery, delivers HBOT-saturated plasma to the outer retinal layers, from which oxygen diffuses inward. documented reversal of retinal ischaemia with HBOT in CRAO patients — demonstrating measurable improvement in visual function in patients treated within the ischaemic window.
| CRAO Treatment Window | Hadanny A et al. (Clinical Ophthalmology, 2016) — case series documenting reversal of retinal ischaemia with HBOT in CRAO. Improvement in visual acuity and retinal perfusion was demonstrated in patients treated within the ischaemic window. The critical variable in every case: time to treatment. Every hour of delay reduces the proportion of recoverable retinal tissue. |
What to Do if Sudden Vision Loss Occurs
- Call emergency services immediately — do not wait to see if vision returns
- Tell the treating team it may be CRAO — ask specifically about HBOT availability
- The nearest hyperbaric facility should be identified and transport arranged immediately
- Standard CRAO interventions can be performed in parallel — they do not preclude HBOT
- Time elapsed since vision loss must be accurately documented — this determines treatment decisions
The HBOT Protocol for Acute Arterial Insufficiency
Standard Parameters — Acute Phase
- Pressure: 2.0 to 2.4 ATA — higher pressures produce greater plasma oxygenation
- Session duration: 90 minutes of pure oxygen breathing
- Frequency in acute phase: 3 sessions in the first 24 hours — every 6 to 8 hours
- Subsequent days: twice daily until vascular repair is achieved and tissue viability is confirmed
- CRAO protocol: initiating HBOT within the first 90 minutes produces the strongest evidence; up to 24 hours may still benefit, though effect diminishes with delay
| FDA Protocol | The US FDA recognises acute peripheral arterial insufficiency as an HBOT indication. The formal protocol specifies sessions three times in the first 24 hours, then twice daily — reflecting the time-critical nature of ischaemic tissue management. HBOT is adjunctive to vascular surgery and intervention, not a replacement. |
Acute Arterial Insufficiency and HBOT in India
India’s burden of acute arterial events is substantial — driven by high rates of atrial fibrillation, rheumatic heart disease (a major source of peripheral emboli), diabetes, and tobacco-related arterial disease. Acute limb ischaemia, CRAO, and post-traumatic arterial compromise represent significant clinical volumes across Indian vascular and ophthalmology departments.
The critical gap is not clinical — Indian vascular surgeons are well-trained in embolectomy and bypass procedures. The gap is in the bridging phase: the hours between arterial event and surgical intervention when HBOT could preserve the tissue that surgery will ultimately try to save.
HBOT for acute arterial insufficiency requires a hyperbaric facility within emergency transport distance. For most Indian patients outside major metros, this does not currently exist. For patients in Delhi NCR, Mumbai, Bangalore, Hyderabad, and Chennai, hospital-based hyperbaric units are accessible within emergency timeframes.
For HBOT facility locations in India, see our guides to HBOT in Delhi and HBOT in Bangalore. For cost and pricing context, visit our HBOT cost guide.
For patients with diabetes and peripheral vascular disease — a primary risk group for acute arterial events — our detailed guide on HBOT for diabetic foot wounds covers the overlapping vascular and wound healing evidence.
Frequently Asked Questions
1. Can HBOT replace surgery for acute arterial insufficiency?
No. HBOT is a bridging therapy — it preserves tissue viability during the window when surgery is being arranged. The blocked artery must be reopened through surgical or endovascular intervention. HBOT cannot achieve this. What it does is change what the surgeon finds when they operate — more viable tissue, less established necrosis, better reconstruction options. The combination of HBOT bridging followed by definitive vascular repair produces the best outcomes.
2. How quickly does HBOT need to start after an arterial event?
As soon as the diagnosis is established and the patient can be safely transported to a chamber. For CRAO, the evidence supports the strongest benefit within 90 minutes of symptom onset — though benefit may extend to 24 hours. For peripheral arterial insufficiency, the 4 to 6 hour ischaemia window for skeletal muscle is the primary reference. Every hour of delay reduces the proportion of tissue that can be saved.
3. Is HBOT safe alongside anticoagulation for arterial embolism?
Yes. Anticoagulation — heparin infusion or oral anticoagulants — is compatible with HBOT. The chamber environment does not interfere with anticoagulant therapy, and anticoagulation does not affect HBOT’s oxygen delivery mechanism. The clinical team should review all medications before chamber entry, as certain interactions exist, but anticoagulation is routinely managed in HBOT patients.
4. Can HBOT help after vascular surgery — not just before?
Yes — and this is an important application that extends beyond the bridging role. Post-revascularisation HBOT addresses the reperfusion injury that occurs when blood flow is restored. The inflammatory cascade triggered by reoxygenation can cause secondary tissue damage even after a technically successful surgical repair. HBOT’s anti-inflammatory mechanisms reduce this secondary injury, supporting better post-operative tissue recovery.
5. Is CRAO always an emergency?
Yes, without exception. Any sudden painless loss of vision in one eye should be treated as a potential CRAO until proven otherwise. The retinal ischaemia window is shorter than any other tissue in the body. Going home to see if vision improves, waiting for a routine ophthalmology appointment, or presenting to a GP rather than an emergency department — these delays can mean permanent vision loss in cases that were recoverable. CRAO is a same-hour emergency.
6. Where can I find HBOT for vascular emergencies in India?
For a comprehensive guide to HBOT facilities across Indian metros, visit our HBOT clinics and locations section. For insurance and coverage guidance, see our HBOT insurance in India guide.
The Bridge Exists. The Window Is Now.
Acute arterial insufficiency is a condition where the outcome is determined by what happens in the hours between the event and the intervention. Surgery is the solution. HBOT is the bridge that keeps tissue viable long enough to reach it.
The physics of plasma oxygenation are not complex. The clinical evidence is not ambiguous. The protocol is established and FDA-recognised. What determines outcomes is whether patients and their families know HBOT exists, whether the treating team knows to ask for it, and whether a chamber is accessible within the critical window.
For CRAO patients especially: sudden vision loss is not something to monitor at home. It is an emergency. And an HBOT chamber reached within 90 minutes can be the difference between recovery and permanent blindness.
For the mechanism of how HBOT delivers oxygen through plasma — the physics behind why it works in vascular emergencies — read our complete guide at How HBOT Works.
For the full conditions evidence base, explore our HBOT conditions reference.
The tissue is alive. The window is open. HBOT keeps it that way until surgery can do the rest.



4 Comments
Comments are closed.


[…] To understand the plasma oxygenation mechanism that makes HBOT effective in vascular emergencies, read our guide on acute arterial insufficiency and HBOT. […]
[…] HBOT for severe anaemia is available at hospital-based hyperbaric units across major Indian metros. For facility information see our guides to HBOT in Delhi and HBOT in Bangalore. For the related plasma oxygenation mechanism, see our article on acute arterial insufficiency and HBOT. […]
[…] For the related review evidence in acute arterial insufficiency — which shares the ischaemia-reperfusion mechanism — see our article on HBOT for acute arterial insufficiency. […]
[…] the primary arterial insufficiency protocol and evidence, see our guide on HBOT for acute arterial insufficiency. For the complete mechanism explanation, visit How HBOT […]