
The Wound That Would Not Heal — And the Science That Changed Everything
In a 2025 systematic review of 391 patients, HBOT consistently reduced major amputation rates and improved wound healing compared to standard care alone.
hbot for diabetic foot — hyperbaric oxygen therapy wound healing
The dressing gets changed. Again.
The wound looks the same. Again. And somewhere, quietly, a fear starts to grow — not just about the wound, but about what might happen if it never heals.
If you are managing a diabetic foot wound — or caring for someone who is — you already know this feeling. The routine of wound care that goes on for weeks, then months. The appointments that produce incremental updates but no resolution. The silent arithmetic of what could happen next.
This is not a failure of effort. It is a failure of oxygen.
Diabetic foot ulcers do not heal the way other wounds do because the tissue beneath them is oxygen-starved. Standard wound care is designed for wounds that have adequate circulation. Yours does not. And no amount of dressing changes, debridement, or topical treatment fully addresses the root biological problem.
Hyperbaric Oxygen Therapy (HBOT) does. Not as a miracle. Not as a guarantee. But as an evidence-backed therapy that addresses the mechanism every other treatment leaves untouched.
What Is HBOT — and Why Does It Work for Diabetic Wounds
HBOT stands for Hyperbaric Oxygen Therapy. It involves breathing 100% pure oxygen inside a pressurised chamber at 1.5 to 2.4 times normal atmospheric pressure.
At that pressure, something changes in your blood that cannot happen under normal conditions.
Normally, oxygen is carried exclusively by your red blood cells. Blood plasma — the liquid portion — carries almost none. That is why reduced circulation in a diabetic foot wound is so damaging: the red blood cells cannot reach the tissue in sufficient numbers, and no oxygen arrives.
HBOT changes this equation entirely. Under therapeutic pressure, oxygen dissolves directly into blood plasma. It does not need red blood cells to carry it. It floods the plasma, and from there it diffuses into the tissue through whatever pathway exists — reaching areas that compromised circulation simply cannot reach.
The mechanism was documented by , whose landmark review established that HBOT triggers multiple biological repair cascades simultaneously — not just oxygenation, but new blood vessel formation, stem cell mobilisation, and reduction of inflammatory markers.
Why Diabetic Wounds Stall — The Oxygen Problem Explained
Diabetes damages blood vessels over time. The small vessels that supply peripheral tissue — particularly in the feet — narrow, harden, and lose their ability to deliver oxygen efficiently. The result is a zone of chronic hypoxia: tissue that is alive but oxygen-deprived, unable to mount the biological responses that healing requires.
Every stage of wound healing depends on oxygen.
- The inflammatory phase — immune cells use oxygen to kill bacteria and clear dead tissue
- The proliferative phase — fibroblasts use oxygen to produce collagen, the structural protein that closes wounds
- The remodelling phase — new blood vessel growth (angiogenesis) requires oxygen as a signalling trigger
When tissue oxygen is below the threshold these processes need, the wound stalls. It does not close. It does not progress. It simply persists — and progressively deepens the risk.
— published in an Indian medical journal — confirmed that HBOT delivers measurable improvements in wound healing in precisely this context, by restoring the oxygen gradient that the wound cannot generate on its own.
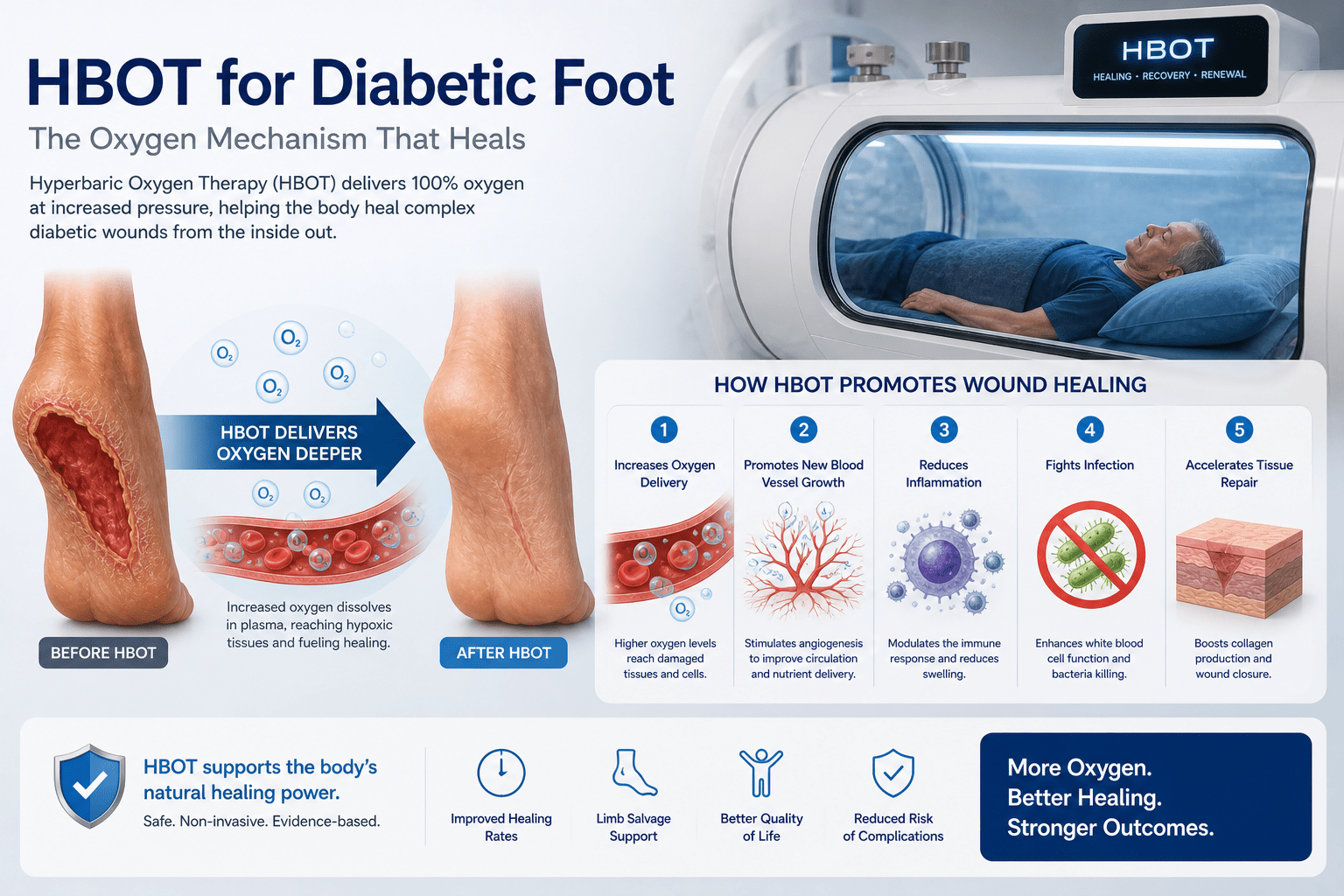
hbot for diabetic foot — oxygen mechanism wound healing diagram
What HBOT Does That Standard Care Cannot
Plasma Oxygenation — Bypassing Compromised Circulation
This is the core mechanism. At 2.0 ATA, dissolved oxygen in blood plasma increases approximately 20-fold compared to breathing normal air. The tissue does not need functional small vessel circulation to receive this oxygen — it arrives through diffusion, driven by the pressure gradient between plasma and the hypoxic tissue.
The wound receives the oxygen it has been denied. The biological processes that have been stalled begin again.
Angiogenesis — Building New Blood Vessels
HBOT triggers a paradoxical but well-documented response: the hyperoxic-hypoxic cycle created by sessions of high-pressure oxygen followed by return to normal conditions stimulates the body to grow new blood vessels.
This was confirmed by , who established that HBOT stimulates vasculogenic stem cell growth and differentiation — the cellular process behind new vessel formation in previously hypovascular tissue.
For a diabetic foot wound, this means something profound: the blood supply that diabetes damaged can be partially rebuilt. Not restored to what it was — but improved enough to sustain ongoing healing where before there was only stagnation.
Stem Cell Mobilisation
A landmark study by demonstrated that HBOT produces an 8-fold increase in circulating stem cells — the body’s own repair cells — by mobilising them from bone marrow into the bloodstream. These cells travel to sites of injury and support tissue regeneration.
For a wound that has exhausted its local repair capacity, this systemic mobilisation provides exactly what is needed: fresh repair resources from a source the wound cannot access on its own.
Anti-Infective Effect
Infected diabetic wounds are a critical complication. HBOT creates a high-oxygen environment that is directly hostile to the anaerobic bacteria most commonly involved in wound infection — the same organisms that drive tissue destruction and systemic risk.
confirmed that HBOT enhances leukocyte bacterial killing capacity — which is impaired in hypoxic tissue — and directly inhibits anaerobic bacterial populations through elevated tissue oxygen tension.
What the Research Shows — Numbers, Not Assertions
The evidence base for HBOT in diabetic foot ulcers is one of the strongest in hyperbaric medicine. Here is what the controlled trial data shows.
Systematic Review — 391 Patients (Cureus, February 2025)
A systematic review published in February 2025, conducting a literature search across PubMed, Scopus, and Web of Science, included six studies with a total of 391 patients. The conclusion was consistent across studies: HBOT reduced major amputation rates, improved ulcer healing rates, and decreased ulcer size and depth compared to standard care alone.
This is the most recent systematic evidence available. The signal is consistent across all included studies.
Meta-Analysis — 768 Patients (Scientific Reports, 2021)
A pooled meta-analysis published in included 14 controlled clinical trials with 768 participants. HBOT was significantly effective in complete healing of diabetic foot ulcers (OR = 0.29; 95% CI 0.14–0.61) and in reduction of major amputation (RR = 0.60; 95% CI 0.39–0.92). The complete healing rate with HBOT was meaningfully higher than with standard care alone.
A risk ratio of 0.60 for major amputation means that patients receiving HBOT had a 40% lower rate of major amputation than those receiving standard care. That is not a marginal finding.
Wagner Grade Stratification — PMC, 2024
A 2024 meta-analysis in the examined HBOT outcomes stratified by diabetic wound severity using the Wagner grading system. Wagner Grade II, III, and IV ulcers — the moderate to severe category — showed higher likelihoods of wound healing with HBOT combined with standard wound treatment.
This matters for Indian patients because the majority of diabetic foot wounds presenting for advanced care are Grade II and above — the exact severity range where the evidence is strongest.
What a Course of HBOT for Diabetic Foot Wounds Looks Like
HBOT is not a single session. It is a cumulative therapy. The biological effects — angiogenesis, stem cell mobilisation, collagen repair — build over a course of sessions. A single visit produces initial oxygenation; the structural repair cascade requires repeated exposure.
For diabetic foot ulcers, standard protocols typically involve:
- 20 to 40 sessions depending on wound severity and clinical response
- 90-minute sessions at 2.0 to 2.4 ATA
- Daily or five-days-per-week frequency
- Assessment of wound response after every 10 to 15 sessions
Wound size, depth, and vascularity are assessed at regular intervals. Progress is measurable — not a matter of opinion. A wound that is not responding within 30 days of HBOT should prompt clinical reassessment.
HBOT is always adjunctive — it works alongside standard wound care, not instead of it. Debridement, infection management, glycaemic control, and offloading all remain essential. HBOT addresses the biological gap that all of these together cannot close.
Who Is a Good Candidate — and Who Should Be Cautious
Strongest Candidates
- Diabetic foot ulcers Grade II and above (Wagner classification)
- Wounds that have not improved after 30 days of standard wound care
- Wounds with clinical or imaging evidence of poor local circulation
- Post-amputation wounds at risk of non-healing
- Diabetic wounds with concurrent osteomyelitis being managed with antibiotics
Situations Requiring Careful Assessment
- Patients with severe chronic obstructive pulmonary disease — lung function must be assessed before treatment
- Patients with untreated pneumothorax — a contraindication
- Patients with claustrophobia — mild cases can be managed, severe cases require individual assessment
- Patients on certain chemotherapy agents — specific interactions require physician review
A qualified HBOT physician should assess every patient before beginning a course. The contraindication list for HBOT is short — but it exists and must be respected.
HBOT for Diabetic Wounds in India — What You Need to Know
India carries the second-largest diabetic population in the world — estimated at 77 million people in 2025. The rate of diabetic foot complications, including non-healing ulcers, is significant and growing.
HBOT for diabetic wounds is available in India at hospital-based hyperbaric units and dedicated wellness HBOT centres in major metros including Delhi NCR, Mumbai, Bangalore, Hyderabad, and Chennai. Costs range from Rs. 3,500 to Rs. 8,000 per session, with full course costs typically between Rs. 70,000 and Rs. 2,50,000 depending on severity and protocol length.
Coverage under Ayushman Bharat and CGHS is possible for specific clinical indications at empanelled hospital-based units — though not universally available.
For detailed information on coverage options, see our guide on .
Frequently Asked Questions
How many HBOT sessions does a diabetic foot wound typically need?
Most diabetic foot ulcer protocols run 20 to 40 sessions. The exact number depends on wound severity, baseline circulation, glycaemic control, and clinical response to the first 10 to 15 sessions. A wound that shows measurable improvement early may complete a shorter course; severe or infected wounds may require longer protocols.
Can HBOT prevent amputation?
The controlled trial evidence shows a 40% reduction in major amputation rates in patients who received HBOT alongside standard care, compared to standard care alone — across 14 controlled trials and 768 participants (Scientific Reports, 2021). HBOT does not guarantee amputation prevention, but the data consistently supports it as a meaningful intervention for patients at risk.
Is HBOT safe for diabetic patients?
Yes — with appropriate pre-treatment assessment. Diabetic patients should have glycaemic control evaluated before beginning HBOT, as sessions can occasionally cause mild hypoglycaemia. Blood sugar monitoring before each session is standard in well-managed protocols. A qualified HBOT physician will assess individual suitability.
Does HBOT work for infected diabetic wounds?
Yes. HBOT has both direct anti-infective properties — creating an oxygen-rich environment hostile to anaerobic bacteria — and indirect effects through enhanced leukocyte killing capacity. For diabetic wounds with concurrent infection, HBOT is typically used alongside antibiotic therapy, not instead of it.
How quickly will I see results?
Some patients report subjective improvement in wound appearance and reduced inflammation within the first 10 sessions. Objective wound measurement — size reduction, depth reduction, improved vascular signals — typically becomes measurable after 15 to 20 sessions. HBOT is cumulative; the biological repair processes it triggers continue to build over the course of treatment and for several weeks after completion.
Is HBOT available for diabetic wounds in Delhi NCR?
Yes. HBOT is available at hospital-based and dedicated wellness centres in Delhi NCR. For a detailed guide, visit our .
You Are Not Out of Options
A wound that has not healed is not a wound that cannot heal.
It is a wound that has not yet had the oxygen it needs to begin the process that standard care alone cannot complete.
HBOT does not work for every patient. No therapy does. But the evidence — across thousands of patients and decades of controlled research — consistently shows that it changes outcomes for the diabetic wounds most likely to reach the stage where amputation becomes the conversation.
The question is not whether the science supports HBOT for diabetic foot wounds. It does. The question is whether you have access to it — and whether you know enough to ask.
To understand how HBOT works at the biological level, visit . For chronic condition applications, read our guide on .
When you are ready to explore what your body is capable of —



7 Comments
Comments are closed.


[…] vascular disease — a primary risk group for acute arterial events — our detailed guide on HBOT for diabetic foot wounds covers the overlapping vascular and wound healing […]
[…] in diabetic wounds — which shares the ischaemic wound bed mechanism — see our detailed guide on HBOT for diabetic foot wounds. For radiation injury healing, see our article on HBOT for radiation […]
[…] For the evidence on HBOT in established diabetic foot wounds — the downstream consequence of unmanaged neuropathy — see our detailed guide on HBOT for diabetic foot wounds. […]
[…] The detailed evidence and treatment protocol for diabetic wound healing is covered in our full guide on HBOT for diabetic foot wounds. […]
[…] the complete diabetic wound evidence, see our guide on HBOT for diabetic foot wounds and our safety guide on HBOT benefits and risks for diabetic […]
[…] the diabetic foot wound healing evidence, see our guides on HBOT for diabetic foot wounds and hyperbaric therapy for diabetic […]
[…] the related diabetic wound healing evidence, see our guides on HBOT for diabetic foot wounds and hyperbaric therapy for diabetic […]